the trachea and esophagus. Seventy-five percent of affected patients develop symptoms by 1 year of age, often within the first month of life and rarely after 6 months of age. Stridor, a nonproductive cough, or a hoarse cry may be noted soon after birth. The stridor generally worsens with feedings, especially solid foods. The cough is characterized as a “seal bark” or “brassy cough.” Respiratory distress can lead to choking, cyanosis, and apnea. Vomiting may precede or follow choking. Despite the esophageal compression, most infants with double aortic arch tolerate liquids well and appear well fed.
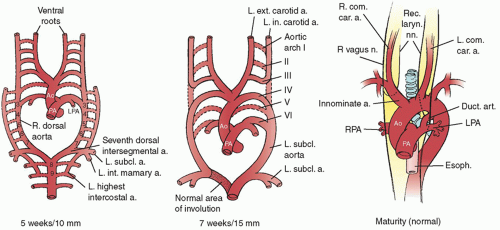 Fig. 78.1. Normal aortic arch development. The normal aortic arch arises from the persistence of the left fourth embryologic arch. Note that the recurrent laryngeal nerve recurs about the derivative of the sixth embryologic arch on the left, that is, the ductus arteriosus, and the derivative of the fourth embryologic arch on the right, that is, the right subclavian artery. This occurs because of the normal involution of the right sixth embryologic arch. a., artery; Ao, aorta; car., carotid; com., common; Duct. art., ductus arteriosus; Esoph., esophagus; ext., external; int., internal; L., left; LPA, left pulmonary artery; n., nerve; PA, pulmonary artery; R., right; Rec. laryn. nn., recurrent laryngeal nerves; RPA, right pulmonary artery; subcl., subclavian. |
Table 78.1 Outcome of the Embryonic Aortic Arches | |||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||
supraclavicular fossa. Infants with the type IB anomaly may also exhibit the compressive symptoms of dyspnea and stridor. Adults more commonly present with dysphagia. Some adults have presented with central nervous system symptoms and the subclavian steal syndrome as a result of stenoses of the left subclavian artery and origin of the vertebral artery.
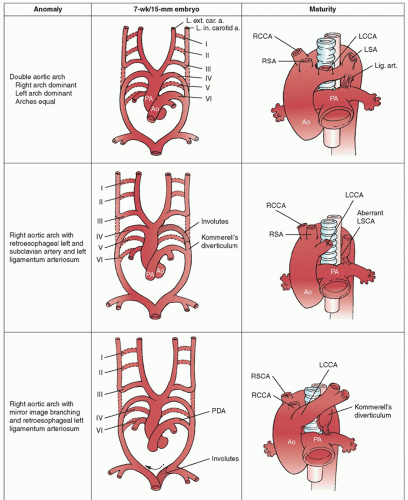 Fig. 78.2. Vascular rings most frequently requiring surgical intervention and their embryologic development. Kommerell’s diverticulum is a remnant of the involuted left fourth aortic arch, which may be the origin of the ductus (ligamentum), the left subclavian artery, or both. a., artery; Ao, aorta; L. ext. car. a., left external carotid artery; L. int. carotid. a., left internal carotid artery; LCCA, left common carotid artery; Lig. art., ligamentum arteriosum; LSA, LSCA, left subclavian artery; PA, pulmonary artery; PDA, patent ductus arteriosus; RCCA, right common carotid artery; RSA, RSCA, right subclavian artery; roman numerals refer to embryologic aortic arches. |
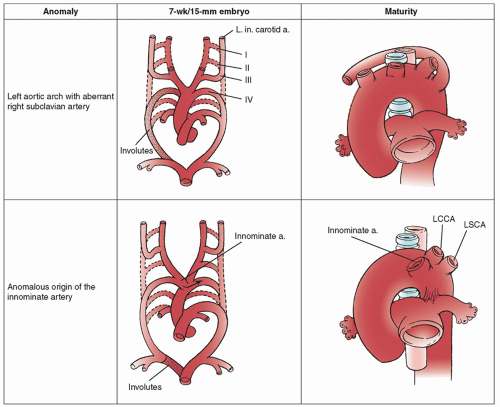 Fig. 78.2. |
but is limited by the need for intravenous contrast and exposure to radiation and may also require sedation for adequate imaging. Rapid, multislice, helical CT scanning (if available) permits rapid scanning with significantly decreased radiation exposure. These scans can be done in <2 seconds in infants, obviating the need for sedation. Aortography is the most invasive technique and is rarely used. It can establish the completeness of a double aortic arch and identify areas of luminal irregularity. It cannot, however, distinguish between a double aortic arch with an atretic segment and a right aortic arch with a retroesophageal ligament. Transthoracic echocardiography is used to detect associated cardiac anomalies and is reasonably sensitive in evaluating vascular rings but appears deficient in determining atretic and nonluminal segments. Echocardiography is important in defining any other associated cardiac anomalies. As mentioned above, these are present in up to 20% of patients and are more common in association with right aortic arch (compared with double aortic arch).
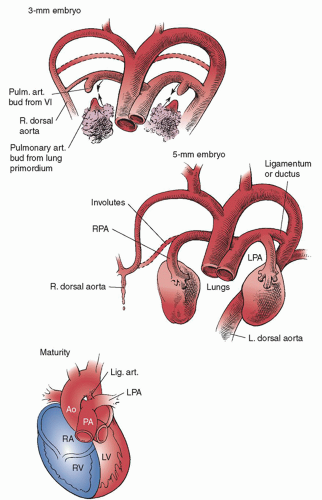 Fig. 78.3. Normal pulmonary artery development. The pulmonary arteries derive from two separate vascular buds, the sixth aortic arches (left and right) and the splanchnic plexus. These buds fuse to form the left and right pulmonary arteries. Ao, aorta; L., left; Lig. art., ligamentum arteriosum; LPA, left pulmonary artery; LV, left ventricle; PA, Pulm. art., pulmonary artery; R., right; RA, right atrium; RPA, right pulmonary artery; RV, right ventricle. |
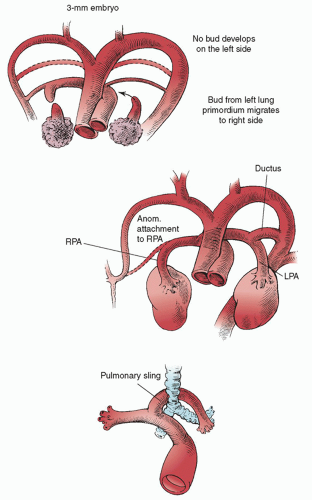 Fig. 78.4. Anomalous development of the left pulmonary artery and formation of the pulmonary artery sling. When the splanchnic bud of the left pulmonary artery fails to fuse with the left sixth aortic arch, it migrates posteriorly between the trachea and esophagus to fuse with the right pulmonary artery. This results in a compressive “sling” about the trachea. Anom., anomalous; LPA, left pulmonary artery; RPA, right pulmonary artery. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


