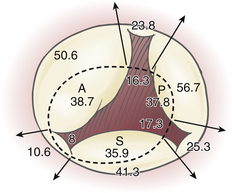
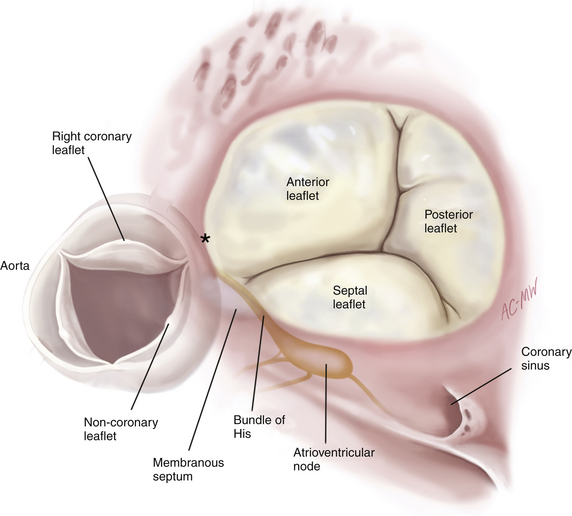
16 The distinction between organic tricuspid regurgitation—where pathology (most commonly rheumatic valve disease, endocarditis, carcinoid valve disease, and trauma) results in structural leaflet damage—and secondary or functional tricuspid regurgitation—where the leaflets appear macroscopically normal—was made in the 1950s. 1 By far the most common reason for tricuspid valve surgery is functional tricuspid regurgitation (TR) in a patient whose primary indication for surgery is mitral valve disease. Functional TR may be due to any combination of right heart dysfunction or dilation, pulmonary hypertension, or left heart dysfunction, and it occurs in the setting of an otherwise normal tricuspid valve. It is commonly seen in patients presenting for mitral, aortic, and coronary bypass surgery, where the indications for concomitant tricuspid repair remain somewhat controversial, and accurate evaluation is complicated by the highly dynamic nature of the dysfunction. Organic tricuspid disease such as endocarditis, carcinoid, and rheumatic valve disease is relatively uncommon in cardiac surgical patients. Functional TR occurs in the absence of pathology affecting the tricuspid valve leaflets. It results from poor leaflet coaptation due to annular dilation and chordal tethering associated with right ventricular dilation and/or left ventricular (LV) dysfunction ( The tricuspid valve maintains its competence through the integrity of its three valve leaflets, the subvalvular apparatus (which consists of thin chordae arising from the RV papillary muscles attaching to the margins and body of the leaflet), and the saddle-shaped valve annulus. 3 Distortion in the three-dimensional geometry of any of these components results in regurgitation. This can be described using Carpentier’s pathophysiologic triad and classification of regurgitation ( Table 16-1). 4 This terminology is most commonly used in reference to the mitral valve but was applied to the tricuspid valve in his original manuscript on the subject and remains a useful nomenclature. Functional TR is due to RV and annular dilation (which cause type I leaflet dysfunction) and/or papillary muscle displacement and leaflet tethering (which cause type IIIb leaflet dysfunction). Both of these mechanisms, which frequently coexist, result in loss of leaflet coaptation and have been described as occurring in three phases: 5 TABLE 16-1 Carpentier’s Classification of Regurgitation, Listing Lesions Commonly Associated with Each Leaflet Dysfunction From Carpentier A, Adams DH, Filsoufi F. Carpentier’s Reconstructive Valve Surgery: From Valve Analysis to Valve Reconstruction. Philadelphia: Saunders; 2010:188. 1. An initial phase in which RV and annular dilation are present, with or without TR 2. Significant TR due to progressive annular and RV dilation 3. Papillary muscle displacement as a result of right and/or LV dysfunction causes leaflet tethering and more severe TR. Annular dilation is an early consequence of RV dilation or dysfunction due to lack of an anatomic fibrous annulus and may increase the annular circumference from around 100 mm to 170 mm. Annular dilation does not occur symmetrically; the posterior and anterior annulus—which are relatively unsupported—dilate more rapidly than the septal annulus ( Fig. 16-1). Structures in close proximity to the tricuspid annulus, and that may be compromised by disease processes or tricuspid valve surgery, include the atrioventricular conduction tissue that lies at the apex of the triangle of Koch (formed by the coronary sinus, septal annulus, and tendon of Todaro), the midportion of the right coronary artery, and the noncoronary cusp of the aortic valve ( Fig. 16-2). Figure 16-1 Segmental dimensions in millimeters are reported for normal (dotted line) and pathologic conditions. Note greater tendency of anterior (A) and posterior (P) annulus to dilate compared to septal (S) annulus. (Adapted from Deloche A, Guerinon J, Fabiani JN. Etude anatomique des valvulopathies rhumatismales tricuspidiennes: application à l’étude des différentes valvuloplasties. Ann Chir Thorac Cardiovasc. 1973;12:343-349.) Figure 16-2 Surgeon’s view of tricuspid valve and coronary sinus, showing anatomic structures close to tricuspid annulus. Asterisk denotes commissure between right and noncoronary aortic sinuses. (From Carpentier A, Adams DH, Filsoufi F. Carpentier’s Reconstructive Valve Surgery: From Valve Analysis to Valve Reconstruction. Philadelphia: Saunders; 2010:178.) Severe left-sided cardiomyopathy and valvular heart disease are usually characterized by elevated left atrial filling pressures that are directly transmitted to the pulmonary vasculature. Pulmonary hypertension is due to a combination of the resultant increased afterload and compensatory pulmonary vasoconstriction and chronic vascular remodeling, resulting in RV pressure overload, which may directly result in TR. Pulmonary hypertension appears to determine the degree of secondary TR to a limited extent, but the relationship is not a direct one. 6 The finding that functional TR may also develop in the absence of demonstrable pulmonary hypertension suggests additional underlying mechanisms. Annular dilation results in loss of leaflet coaptation, causing type I regurgitation, and has been shown to be a strong independent predictor of functional TR. 6 It has more recently become apparent that in addition to dilation, several other annular abnormalities characterize functional TR. Three-dimensional (3D) echocardiography has been used to show how valves with functional TR lose their normal saddle-shaped annular geometry, becoming flattened and circular as they dilate, with an associated asymmetric loss of annular contraction. 6 Leaflet tethering that results in Carpentier type IIIb regurgitation may be the result of chordal or papillary muscle shortening or papillary muscle displacement, most commonly due to ventricular dilation. Functional TR due to septal leaflet tethering may be observed in the context of normal RV function, dimensions, and pulmonary pressure. This really leaves only LV pathology as a potential explanation for functional TR in this setting. The right and left ventricles are interdependent at the septum, where the papillary muscles giving rise to the chordae of the tricuspid valve’s septal leaflet take origin. Where LV pathology results in a dysfunctional or displaced interventricular septum, tethering of the septal tricuspid leaflet may result, even if the RV appears echocardiographically normal.7,8 This may be why LV dysfunction is associated with functional TR. In an analysis of 75 patients with dilated RVs, eccentricity of the RV and tricuspid valve tethering area were most strongly predictive of the severity of functional TR, whereas RV function, dimension, and pulmonary artery pressures were insignificant determinants. 9 Organic tricuspid disease requiring surgery is uncommon ( Table 16-2). Right-sided infective endocarditis is suggestive of intravenous drug use but is also seen in patients with indwelling catheters for dialysis or chemotherapy. Multiple vegetations attached to indwelling catheters and wires and extending over the atrial and ventricular surfaces of the leaflets, which are frequently thickened, are common; leaflet perforations and annular abscesses less so. Trauma can cause TR, most commonly as a result of iatrogenic mechanisms such as endomyocardial biopsies in heart transplant patients, fibrosis around pacing wires, or extraction of long-term intracardiac lines. Blunt trauma is an unusual cause of TR due to papillary muscle rupture ( TABLE 16-2 Indications for Intervention in Tricuspid Valve Disease RV, Right ventricular; TR, tricuspid regurgitation; TS, tricuspid stenosis. ∗Percutaneous technique can be attempted as a first approach if TS is isolated. From Vahanian A, Baumgartner H, Bax J, et al. Guidelines on the management of valvular heart disease: the Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology. Eur Heart J. 2007;28:230-268. Severe symptomatic TR is an American College of Cardiology/American Heart Association (ACC/AHA) and European Society of Cardiology class I indication for surgical intervention ( Boxes 16-1 and 16-2).10
Tricuspid Valvular Disease
 Overview
Overview
 Functional Tricuspid Regurgitation
Functional Tricuspid Regurgitation
 Video 16-1): the most common underlying pathophysiology is congestive heart failure, followed by pulmonary hypertension and aortic or mitral valve dysfunction. It is a common finding in severe ischemic and dilated cardiomyopathy. Significant functional TR is found in up to a third or more of patients presenting for mitral surgery. 2 Although severe TR is a widely accepted indication for surgical intervention, moderate TR is highly dynamic, and its impact on prognosis and functional capacity is not well defined. Indications and optimal strategy for treatment of moderate functional TR at the time of concomitant cardiac surgery remain controversial.
Video 16-1): the most common underlying pathophysiology is congestive heart failure, followed by pulmonary hypertension and aortic or mitral valve dysfunction. It is a common finding in severe ischemic and dilated cardiomyopathy. Significant functional TR is found in up to a third or more of patients presenting for mitral surgery. 2 Although severe TR is a widely accepted indication for surgical intervention, moderate TR is highly dynamic, and its impact on prognosis and functional capacity is not well defined. Indications and optimal strategy for treatment of moderate functional TR at the time of concomitant cardiac surgery remain controversial.
 Functional Anatomy
Functional Anatomy
Valve Dysfunctions
Lesions
Type I: Valve dysfunction with normal leaflet motion
Annular dilation and deformation
Leaflet perforation
Type II: Leaflet prolapse
Chordae rupture
Chordae elongation
Papillary muscle rupture
Papillary muscle elongation
Type III: Restricted leaflet motion
IIIa: Diastolic
Leaflet thickening and retraction
Commissure fusion
Chordae thickening
Chordae fusion
Calcification
IIIb: Systolic
Ventricular aneurysm
Ventricular fibrous plaque
Ventricular dilation
Leaflet entrapment
 Pathophysiology
Pathophysiology
Pulmonary Hypertension
Annular Dilation
Leaflet Tethering
 Organic Tricuspid Disease
Organic Tricuspid Disease
 Video 16-1). Rheumatic valve disease, rheumatoid arthritis, systemic lupus erythematosus, and antiphospholipid syndrome are all associated with organic leaflet lesions that may result in significant tricuspid valve dysfunction. Rheumatic tricuspid valve disease is often predominantly functional, but it is occasionally characterized by leaflet involvement with thickened, shortened leaflets and commissural fusion. Carcinoid valve disease usually involves the tricuspid and pulmonary valve, causing very pronounced leaflet thickening and mixed stenotic and regurgitant lesions (regurgitation is usually predominant). In these patients, one of the goals of valve surgery is to facilitate subsequent resection of hepatic metastases. Tricuspid valve stenosis, which is predominantly caused by rheumatic valve disease and occasionally a feature of carcinoid valve disease, is an extremely rare entity in developed countries.
Video 16-1). Rheumatic valve disease, rheumatoid arthritis, systemic lupus erythematosus, and antiphospholipid syndrome are all associated with organic leaflet lesions that may result in significant tricuspid valve dysfunction. Rheumatic tricuspid valve disease is often predominantly functional, but it is occasionally characterized by leaflet involvement with thickened, shortened leaflets and commissural fusion. Carcinoid valve disease usually involves the tricuspid and pulmonary valve, causing very pronounced leaflet thickening and mixed stenotic and regurgitant lesions (regurgitation is usually predominant). In these patients, one of the goals of valve surgery is to facilitate subsequent resection of hepatic metastases. Tricuspid valve stenosis, which is predominantly caused by rheumatic valve disease and occasionally a feature of carcinoid valve disease, is an extremely rare entity in developed countries.
Indication
Class
Severe TR in a patient undergoing left-sided valve surgery
IC
Severe primary TR and symptoms despite medical therapy without severe RV dysfunction
IC
Severe TS (±TR) with symptoms despite medical therapy ∗
IC
Severe TS (±TR) in a patient undergoing left-sided valve intervention ∗
IC
Moderate organic TR in a patient undergoing left-sided valve surgery
IIaC
Moderate secondary TR with dilated annulus (>40 mm) in a patient undergoing left-sided valve surgery
IIaC
Severe TR and symptoms after left-sided valve surgery, in the absence of left-sided myocardial, valve, or RV dysfunction and without severe pulmonary hypertension (systolic pulmonary artery pressure >60 mmHg)
IIaC
Severe isolated TR with mild or no symptoms and progressive dilation or deterioration of RV function
IIbC
 Indications for Tricuspid Valve Surgery
Indications for Tricuspid Valve Surgery
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Thoracic Key
Fastest Thoracic Insight Engine
