Table 13.1 Diseases of the Tricuspid and Pulmonary Valves | |||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||
This phenomenon is dependent on mechanical atrial systole and is not present in atrial fibrillation. It is also dependent on relatively low pulmonary artery diastolic pressures so that atrial contraction creates the driving force for partial opening of the pulmonary valve. The pulmonary valve leaflet then moves posteriorly (in a patient in supine position), that is, away from the transducer during systole. It is not uncommon for visualization to be incomplete throughout the entire cardiac cycle and for only the A wave and opening slope of the pulmonary valve to be detectable. With excellent acoustic windows, the full opening of the pulmonary valve and the degree to which it remains in a fully open position during systole can occasionally be appreciated (Fig. 13.8) and its subsequent closure in diastole also noted.
Table 13.2 Appropriateness Criteria for Use of Echocardiography in Pulmonic Tricuspid Valve Disease | |||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||
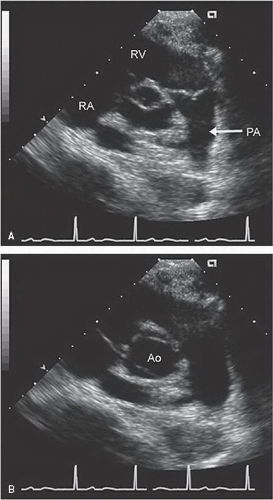 FIGURE 13.1. Transthoracic parasternal short-axis view at the base of the heart visualizing the pulmonary valve. Notice the central closure point in diastole (A) and the inability to visualize the normal leaflets that are fully open in systole (B). |
M-mode echocardiography. Figure 13.9 schematizes the appropriate sample volume position and provides an example of a normal pulsed Doppler imaging of pulmonary flow. It should be emphasized that many of the indirect parameters of right heart hemodynamics that can be derived from the pulmonary outflow tract spectral profile are dependent on optimal imaging planes, including the central position of the sample volume within the pulmonary artery (as opposed to recording it along the periphery) and recording at a level just distal to the tips of the pulmonary valve. The normal pulmonary outflow tract velocity ranges from 1 to 1.5 m/sec. As with other valves, the time velocity integral of this valve can be determined and in combination with the outflow tract dimension can be used to calculate volumetric flow (Fig. 13.9). Other parameters of the pulmonary outflow tract velocity include acceleration time. Acceleration time is defined as the time in milliseconds from the onset of ejection to peak systolic velocity. In normal individuals, acceleration time exceeds 140 milliseconds and progressively shortens with increasing degrees of pulmonary hypertension (Fig. 13.10).
 FIGURE 13.2. Parasternal short-axis view at the base of the heart with a slightly different angulation than presented in Figure 13.1. In this view, the bifurcation of the pulmonary artery into right and left pulmonary arteries can be visualized (forked arrow). The plane of the pulmonic valve is noted by the horizontal arrow. |
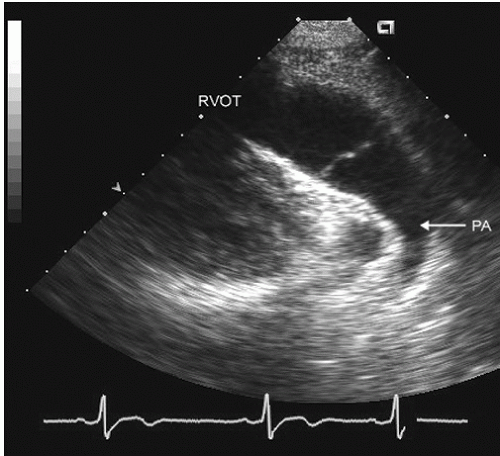 FIGURE 13.3. Parasternal long-axis view of the right ventricular outflow tract, pulmonary artery, and pulmonary valve recorded in diastole. In the real-time image, note the full motion of the valve to the margins of the arterial wall. PA, pulmonary artery. |
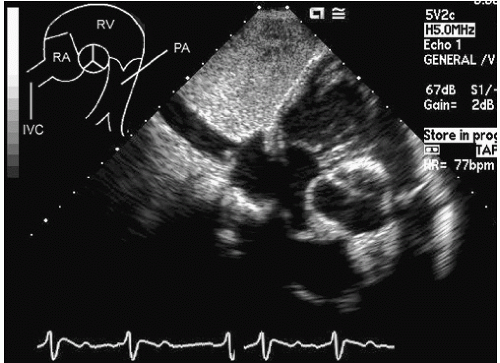 FIGURE 13.4. Subcostal short-axis view of the base of the heart shows a portion of the right atrium, tricuspid valve, right ventricle and outflow tract, pulmonary valve, and pulmonary artery. Structures are as noted on the schematic in the upper left of the figure. |
 FIGURE 13.5. Transesophageal echocardiogram recorded in 55° and 0° views at the base of the heart. A: The right ventricular outflow tract and pulmonary artery are clearly visualized as is the pulmonary valve (PV). B: The pulmonary valve and a larger portion of the main pulmonary artery and right pulmonary artery (RPA) are shown. In this view, it is often difficult to visualize simultaneously the RPA and the left pulmonary artery (LPA). PA, pulmonary artery. |
should be considered a normal variant. These inconsequential jets of pulmonary valve insufficiency may arise centrally or more peripherally at the junction of the valve cusps with the pulmonary artery (Fig. 13.12). When they arise immediately adjacent to the aortic wall, they have been confused for a pathologic communication between the aorta and the pulmonary artery. Recognition of the exclusively diastolic flow should allow avoidance of any confusion.
 FIGURE 13.6. Transesophageal echocardiogram recorded at 76° from a low esophageal position showing the body and outflow tract of the right ventricle, the pulmonary valve in a closed position (arrow) and in the color flow image mild pulmonic insufficiency (arrow). PA, pulmonary artery. |
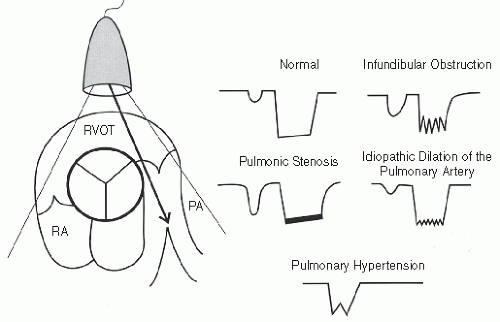 FIGURE 13.7. Schematic representation of M-mode echocardiograms of normal and abnormal pulmonary valves. In the normal schematic, note the normal A wave and boxlike opening of the valve. Various disease states are also schematized. PA, pulmonary artery. |
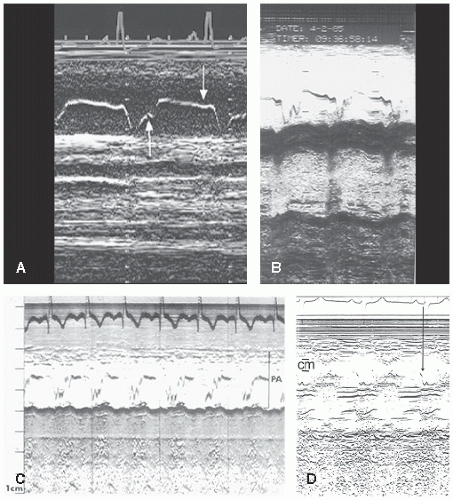 FIGURE 13.8. M-mode echocardiograms recorded in patients with different abnormalities. A: Image recorded in a patient with pulmonary hypertension. Note the loss of the pulmonic valve A wave (downward-pointing arrow) and midsystolic notching (upward-pointing arrow) of the valve. B: Note the low-amplitude biphasic A wave. C: Image recorded in a patient with infundibular obstruction shows coarse fluttering of the valve in systole. D: Image recorded in a patient with pulmonary valve stenosis. Note the accentuated A wave (1 cm). PA, pulmonary artery. |
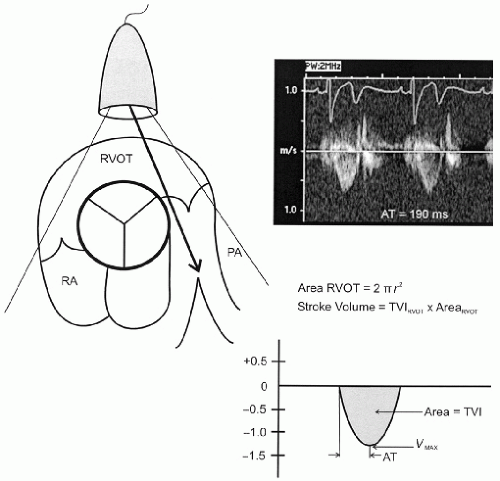 FIGURE 13.9. Schematic representation of the methods for recording pulmonary/right ventricular outflow tract velocities. The parasternal short-axis view is used with the interrogating beam aimed posteriorly along the long axis of the right ventricular outflow tract and proximal pulmonary artery. The spectral display is schematized at the lower right, including its various components such as time velocity ventricle (TVI) and acceleration time (AT). In the upper right is an example of a normal flow profile. The method for calculating stroke volume from these parameters is also displayed. |
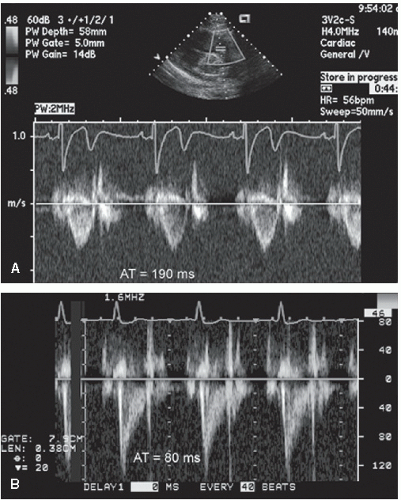 FIGURE 13.10. Spectral flow profiles recorded in a normal individual (A) with an acceleration time (AT) of 190 milliseconds and a patient with significant pulmonary hypertension in whom the acceleration time is 80 milliseconds (B). AT, acceleration time. |
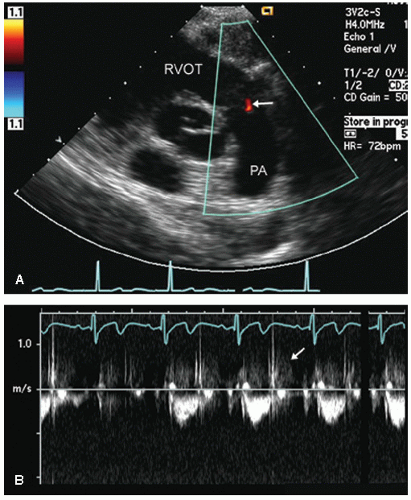 FIGURE 13.11. Parasternal short-axis view at the base of the heart in a normal individual reveals trivial central pulmonary valve insufficiency. A: Note the very small central regurgitant jet (arrow). B: Note the faint early diastolic retrograde Doppler spectral signal consistent with minimal pulmonary insufficiency. |
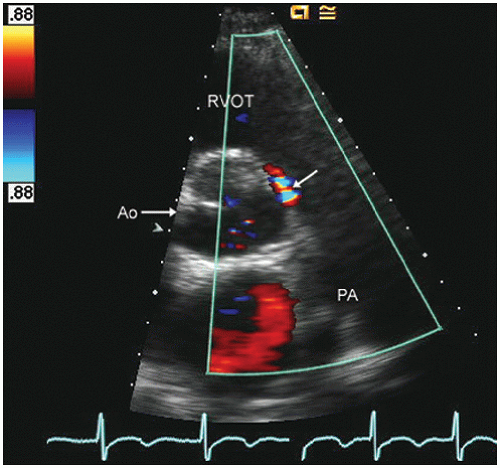 FIGURE 13.12. Parasternal short-axis view recorded at the base of the heart in a patient with minimal pulmonary valve insufficiency originating at the lateral aspect of the cusp commissure. Because this jet originates immediately adjacent to the aorta, it could be confused for an aorta-pulmonary fistula. Note, however, the exclusively diastolic flow, which would not be expected in the presence of the true shunt. |
amplitude (>6 mm) with thickening of the leaflets. The accentuated A wave occurs only in patients in sinus rhythm and is probably dependent on the presence of concurrent right ventricular hypertrophy. It does not allow quantitation of severity, but the presence of an accentuated A wave is indirect evidence of pulmonary valve stenosis. The origin of the accentuated A wave is the relatively elevated right ventricular diastolic pressure in comparison with the pulmonary artery diastolic pressure. With atrial contraction, pressure is transmitted by the hypertrophied noncompliant right ventricle to the pulmonary valve and pulmonary artery. With atrial contraction, right ventricular outflow tract pressure exceeds pulmonary artery diastolic pressure, and there is accentuated presystolic opening of the pulmonary valve. As noted previously, this is a qualitative descriptor implying the presence of pulmonary valve stenosis but provides no quantitative information.
 FIGURE 13.13. Transthoracic echocardiogram recorded in a parasternal short-axis view in a patient with pulmonic stenosis. Note the thickening of the pulmonary valve cusps (arrows) and the continuous wave Doppler velocity of 4.5 m/sec corresponding to a peak pressure gradient across the pulmonary valve of 81 mm Hg. The color Doppler image depicts eccentric acceleration toward the stenotic orifice as well as an eccentric jet in the pulmonary artery. PA, pulmonary artery. |
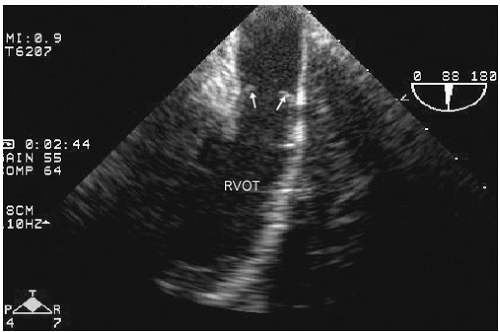 FIGURE 13.14. Transesophageal echocardiogram recorded in an adolescent with congenital pulmonary valve stenosis. This image was recorded in midsystole. Note the thickening of the pulmonary valve leaflets and the doming motion (arrows) characteristic of valvar pulmonary stenosis. (Courtesy of Gregory Ensing, MD.) |
which in turn is a consequence of pulmonary hypertension, also results in pulmonary valve regurgitation. Occasionally, one encounters congenital absence of one or more pulmonary valve cusps, which results in severe pulmonary valve regurgitation.
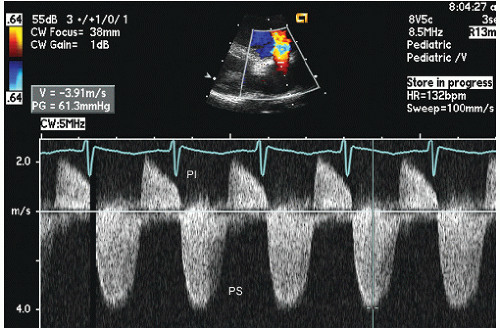 FIGURE 13.15. Continuous wave Doppler imaging through the right ventricular outflow tract and pulmonary valve in a patient with pulmonary valve stenosis. Note the peak pressure gradient of 61 mm Hg and the presence of concurrent pulmonary valve insufficiency. PI, pulmonary valve insufficiency; PS, pulmonary valve stenosis. |
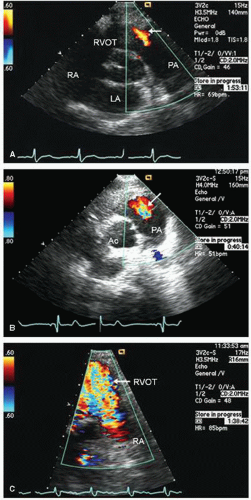 FIGURE 13.16. Parasternal short-axis view color Doppler flow images recorded in patients with mild (A), moderate (B), and severe (C) pulmonary valve insufficiency. PA, pulmonary artery. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


