Chapter 19 Sudden Cardiac Arrest and Sudden Cardiac Death
Please go to expertconsult.com for supplemental chapter material.
Clinical Aspects of Cardiac Arrest
Key Point
The absence of pulses in an unresponsive individual is the major diagnostic sign of cardiac arrest.
When cardiac arrest is recognized, cardiopulmonary resuscitation (CPR) efforts must be started without delay. The latest (2010) recommendations for the general public in the initial basic life support treatment of a witnessed cardiac arrest involve an approach of effective, continuous chest compressions without interruption for mouth-to-mouth resuscitation (so-called hands-only resuscitation). These new recommendations (Box 19-1) are designed to improve the practice of resuscitation in untrained bystanders; they apply to adults, children, and infants but exclude newborns.
BOX 19-1 Cardiopulmonary Resuscitation (CPR) Guidelines
Bystanders Trained in CPR
2. Deliver 30 forceful, manual chest compressions of the sternum, at a rate of 100 compressions per minute and at a depth of approximately 2 inches.
3. Open the airway with a head tilt and chin lift.
4. Perform CPR with a 30:2 sternal compression to breath ratio.
5. Continue until paramedics arrive or the victim becomes responsive.
• Unresponsive infants and young children
• Adult victims who are found already unconscious and not breathing normally
Basic ECG Patterns in Cardiac Arrest
The three basic ECG patterns seen with cardiac arrest were mentioned in earlier chapters. Cardiac arrest may be associated with the ECG patterns listed in Box 19-2.
BOX 19-2 Three Basic ECG Patterns with Cardiac Arrest
• Ventricular tachyarrhythmia, including ventricular fibrillation (VF) or a sustained type of pulseless ventricular tachycardia (VT)
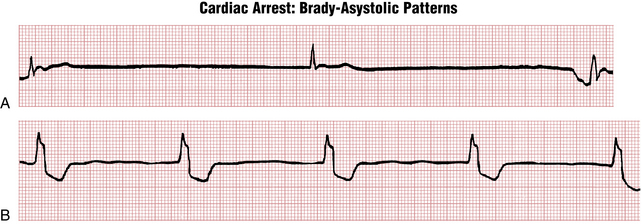
• Ventricular asystole or a brady-asystolic rhythm with an extremely slow rate
• Pulseless electrical activity (PEA), also referred to as electromechanical dissociation (EMD)
The ECG patterns seen in cardiac arrest are briefly reviewed in the following sections, with emphasis placed on their clinical implications (Figs. 19-1 to 19-6).

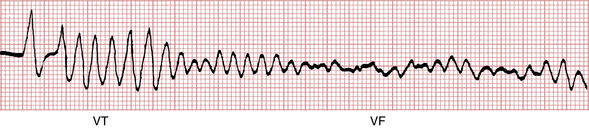

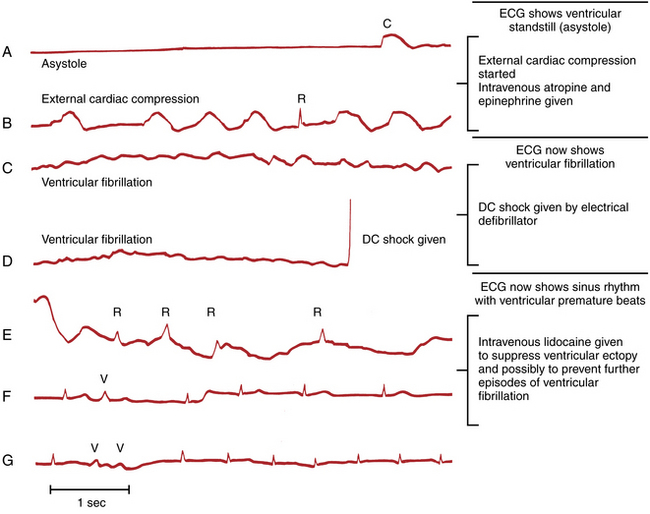
Figure 19-3 Complete ventricular standstill (asystole) producing a straight-line pattern during cardiac arrest.