Chapter 17 Atrioventricular Conduction Abnormalities Delays, Blocks, and Dissociation Syndromes
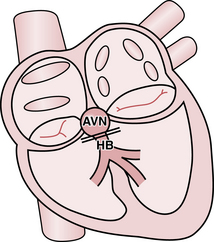
With normal cardiac anatomy (see Chapter 1), the only means of electrical communication between the atria and ventricles is via the specialized conduction system of the heart. This relay network comprises the atrioventricular (AV) node, which is connected to the His bundle, which in turn is connected to the bundle branches (Fig. 17-1). The atria and ventricles are otherwise electrically isolated from each other by connective tissue in the indented rings (grooves) between the upper and lower chambers. The key exception occurs with Wolff-Parkinson-White (WPW) preexcitation syndrome, described in Chapters 12 and 14.
The slight physiologic delay, reflected in the normal PR interval, between atrial and ventricular activation allows the ventricles optimal time to fill with blood during and after atrial contraction. Excessive slowing or actual interruption of electrical signal propagation across the heart’s conduction system is abnormal and termed AV (atrioventricular) block or heart block. The closely related (and often confusing to students and experienced clinicians!) topic of AV dissociation is discussed at the end of this chapter and in Chapter 10.
What is the Degree of AV Block?
Depending on the severity of conduction impairment, there are three major degrees of AV block:
• First-degree (PR interval prolongation): uniform slowing of conduction between the atria and ventricles (an increase in the normal AV delay described earlier), but without its interruption
• Second-degree: intermittent interruption of conduction, which may be further designated as Mobitz I (AV Wenckebach) or Mobitz II varieties
• Third-degree: complete interruption of AV conduction, with a nodal or infranodal escape rhythm, or with asystole
Two other important subtypes of second-degree AV block, namely 2:1 block and high-grade block (also referred to as “advanced second-degree AV block”) will also be discussed.
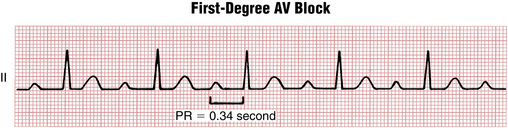
Prolonged PR Interval (First-Degree AV Block)
First-degree AV block (Fig. 17-2) is characterized by a P wave (usually sinus in origin) followed by a QRS complex with a uniformly prolonged PR interval greater than 200 msec. The preferred term is PR interval prolongation because the signal is not really blocked, but rather it is delayed. The PR interval can be slightly prolonged (e.g., 240 msec) or it can become markedly long (up to 400 msec or longer).
Second-Degree AV Block Syndromes
With Mobitz type I, the classic AV Wenckebach pattern (Figs. 17-3 and 17-4), each stimulus from the atria has progressive difficulty traversing the AV node to the ventricles (i.e., the node becomes increasingly refractory). Finally, the atrial stimulus is not conducted at all, such that the expected QRS complex is blocked (“dropped QRS”). This cycle is followed by relative recovery of the AV junction, and then the whole cycle starts again.
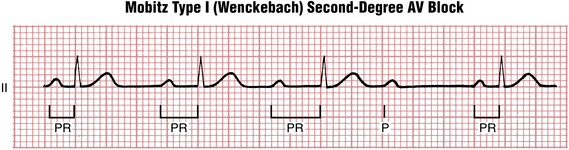
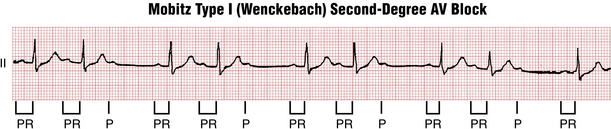
The number of P waves occurring before a QRS complex is “dropped” may vary. The nomenclature is in terms of a ratio that gives the number of P waves to QRS complexes in a given cycle. The numerator is always one higher than the denominator. In many cases just two or three conducted P waves are seen before one is not conducted (e.g., 3:2, 4:3 block). In other cases, longer cycles are seen (e.g., 5:4, 10:9, etc.).∗
As you can see from the examples, the Wenckebach cycle also produces a distinct clustering of QRS complexes separated by a pause (the dropped beat). Any time you encounter an ECG with this type of group beating, you should suspect AV Wenckebach block and look for the diagnostic pattern of lengthening PR intervals and the presence of a nonconducted P wave. As discussed in the following text, infranodal second-degree AV block (Mobitz type II) also demonstrates grouped beating with dropped QRS complexes, but without significant progressive PR interval prolongation (Fig. 17-5).

Figure 17-5 Mobitz type II atrioventricular (AV) second-degree heart block. Lead V1 recording shows sinus rhythm (P wave; arrows) at a rate of about 75 beats/min (with left atrial abnormality). Most important, note the abrupt appearance of sinus P waves that are not followed by QRS complexes (nonconducted or “dropped” beats). Furthermore, the PR interval before the nonconducted P wave and the PR of the beat after (about 0.14 sec) are the same. This finding contrasts with AV Wenckebach with 3:2 or higher ratios of conduction in which the PR interval after the nonconducted beat is noticeably shorter than the one before (see Figs. 17-3 and 17-4). The QRS of the conducted beats is also wide because of a left ventricular conduction delay. Mobiz II block is often associated with bundle branch abnormalities because the conduction delay is infranodal. Finally, note that the intermittent AV conduction pattern here gives rise to “group beating,” also a feature of AV Wenckebach block.
Caution! Be careful not to mistake group beating due to blocked atrial premature beats (APBs) for second-degree AV block. In the former, the nonconducted P waves come “early”; in the latter they come “on time” (see Chapter 14).
A subset of second-degree heart block occurs when there are multiple consecutive nonconducted P waves present (e.g., P-QRS ratios of 3:1, 4:1, etc.). This finding is referred to as high-degree (or advanced) AV block. It can occur at any level of the conduction system (Fig. 17-6). A common mistake is to call this pattern Mobitz II block.

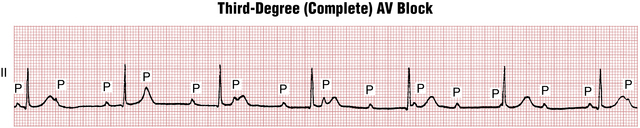
Third-Degree (Complete) AV Block
First- and second-degree heart blocks are examples of incomplete block because the AV junction conducts some stimuli to the ventricles. With third-degree, or complete, heart block, no stimuli are transmitted from the atria to the ventricles. Instead, the atria and ventricles are paced independently. The atria often continue to be paced by the sinoatrial (SA) node. The ventricles, however, are paced by a nodal or infranodal escape pacemaker located somewhere below the point of block. The resting ventricular rate with complete heart block may be around 30 beats/min or lower or as high as 50 to 60 beats/min. This situation, when there is no “cross-talk” between the atria and ventricles and each of them is driven independently by a separate pacemaker at a different rate, is one example of AV dissociation. In the setting of complete heart block, AV dissociation almost always produces more P waves than QRS complexes (Box 17-1). However, as discussed later, AV dissociation is not unique to complete heart block.
BOX 17-1 ECG with Sinus Rhythm and Complete Heart Block: Three Key Features
• P waves (upright in lead II) are present, with a relatively regular sinus rate that is typically much faster than the ventricular rate.
• QRS complexes are present, with a slow (usually near-constant) ventricular rate.
• The P waves bear no relation to the QRS complexes; thus, the PR intervals are variable.
Examples of complete heart block are shown in Figures 17-7 and 17-8.