Chapter 12 Wolff-Parkinson-White Preexcitation Patterns
Wolff-Parkinson-White Pattern: Preexcitation and Bypass Tracts
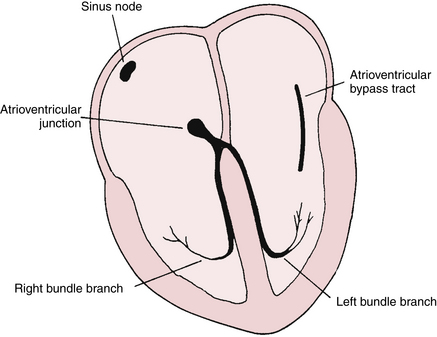
The WPW pattern is a distinctive and important ECG abnormality caused by preexcitation of the ventricles. Normally the electrical stimulus travels to the ventricles from the atria via the atrioventricular (AV) junction. The physiologic lag of conduction through the AV junction results in the normal PR interval of 0.12 to 0.2 sec. Consider the consequences of having an extra pathway between the atria and ventricles that would bypass the AV junction and preexcite the ventricles. This situation is exactly what occurs with the WPW pattern: an atrioventricular bypass tract connects the atria and ventricles, circumventing the AV junction (Fig. 12-1).
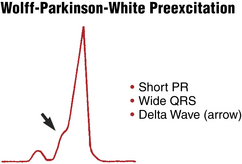
Preexcitation of the ventricles with the classic WPW pattern produces the following characteristic triad of findings on the ECG (Figs. 12-2 to 12-4):
1. The QRS complex is widened, giving the superficial appearance of a bundle branch block pattern. However, the wide QRS is caused not by a delay in ventricular depolarization but by early stimulation of the ventricles. The T wave is also usually opposite in polarity to the wide QRS in any lead, similar to what is seen with bundle branch blocks (“secondary T wave inversions”).
2. The PR interval is shortened (often but not always to less than 0.12 sec) because of the ventricular preexcitation.
3. The upstroke of the QRS complex is slurred or notched. This is called a delta wave.
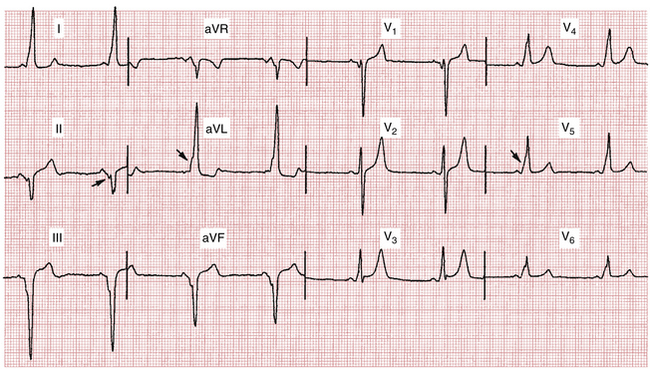
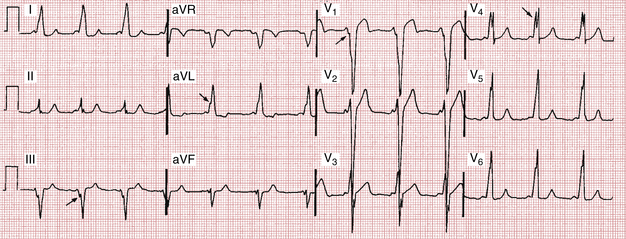
Figures 12-2 and 12-3
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


