Chapter 16 Ventricular Arrhythmias
Please go to expertconsult.com for supplemental chapter material.
Ectopic (nonsinus) depolarizations frequently arise in the ventricles themselves, or the fascicular system, producing premature ventricular beats (or complexes), ventricular tachycardia (VT), discussed later, and in the most electrophysiologically unstable settings, sometimes ventricular fibrillation (VF) leading to immediate cardiac arrest (also see Chapter 19).
Ventricular Premature Beats
Ventricular premature beats (VPBs)∗ are premature depolarizations arising in the ventricles, analogous to atrial premature beats (APBs) and junctional premature beats (JPBs), which are supraventricular in origin. Recall that with APBs and JPBs, the QRS complex is usually of normal (“narrow”) width because the stimulus spreads synchronously through the bundle branches to the ventricles (unless a bundle branch block or some other cause of aberrancy is present).
With VPBs, however, the premature depolarizations typically arise in either the right or left ventricle. Therefore, the ventricles are not stimulated simultaneously, and the stimulus spreads through the ventricles in an aberrant direction and asynchronous way. Thus, the QRS complexes are wide with VPBs, just as they are with the bundle branch block patterns.† Examples of VPBs are shown in Figures 16-1 to 16-8.
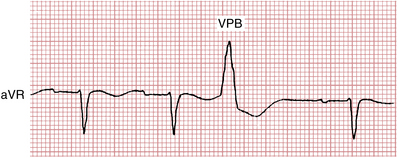
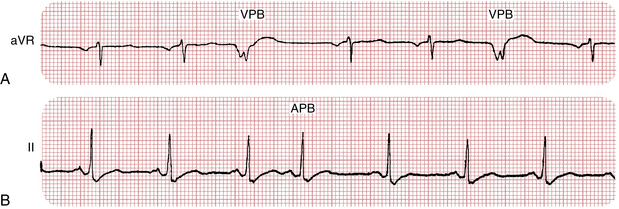
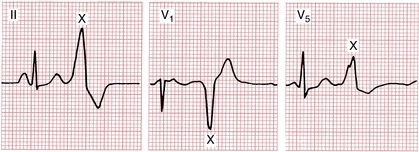
Figure 16-3 Notice that the same ventricular premature beat (marked X) recorded simultaneously in three different leads has different shapes. By comparison, notice that the multiform ventricular premature beats shown in Figure 16-11 have different shapes in the same lead.
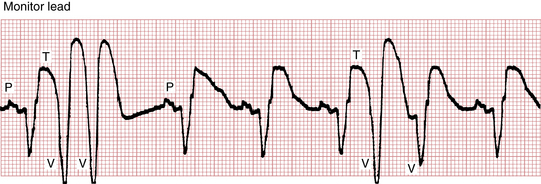
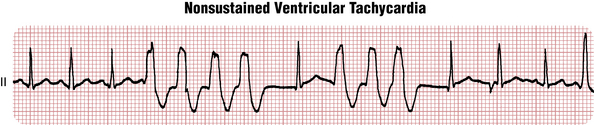
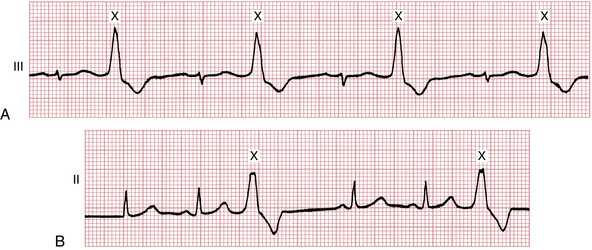
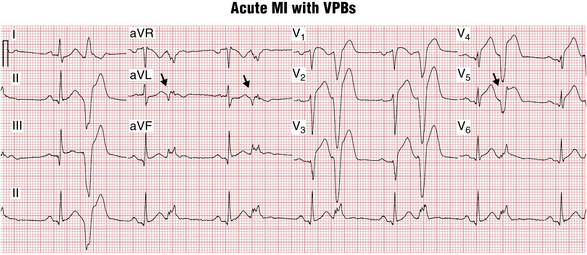
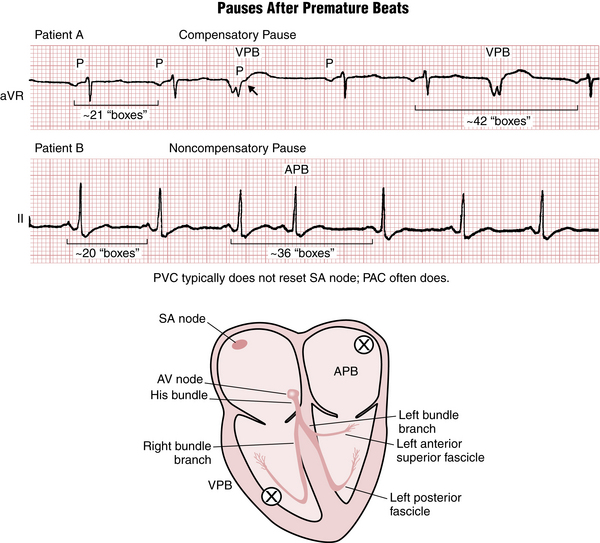
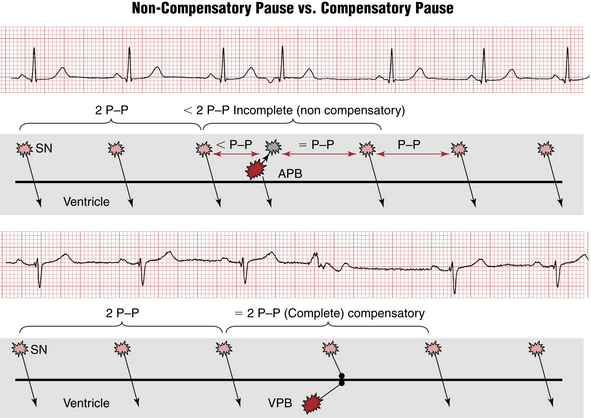
Figure 16-8 Difference between noncompensatory and compensatory pauses after atrial premature beats (APBs) and ventricular premature beats (VPBs), respectively. See text and Figure 16-9.
VPBs most often precede a sinus P wave. (Occasionally they appear just after a sinus P wave but before the normal QRS complex.) Sometimes, VPBs are followed by retrograde (nonsinus) P waves (negative in lead II) that arise because of reverse stimulation (from bottom to top) of the atria by each VPB. This sequence, called “VA” (ventricular-atrial) conduction, is identical to what may occur with ventricular pacing (see Chapter 21).
Features
Clinicians comment on a number of features of VPBs that may have clinical relevance.
Frequency
VPBs may occur in various combinations. Two in a row (see Fig. 16-4) are referred to as a pair or couplet. Three or more in a row are, by definition, VT (see Fig. 16-5). Sometimes, as shown in Figure 16-6A, isolated VPBs occur so frequently that each normal beat is followed by a VPB. This produces a distinctive repetitive grouping of one normal beat and one VPB, which is called ventricular bigeminy (see Figs. 16-6 and 16-7). The sequence of two normal beats with a VPB is ventricular trigeminy. Three normal beats followed by a VPB constitutes ventricular quadrigeminy.
Morphology and Origin
• If the ectopic beat originates in the left ventricle, then right ventricular activation will be delayed and the QRS of the VPB will resemble a right bundle branch block (RBBB).
• If the ectopic beat comes from the right ventricle, then left ventricular activation is delayed, and the QRS shape resembles a left bundle branch block (LBBB) pattern.
• VPBs from the interventricular septum often show an intermediate pattern between RBBB and LBBB. They are usually relatively narrow as both ventricles get activated simultaneously from the middle of the ventricles.
The further away from the middle of the heart VPB origin is, the wider is the QRS. VPBs coming from the top (base) of the heart have “inferior” QRS axis—pointing down and therefore positive in leads II, III, and aVF. They are often called “outflow tract” VPBs because their origin is located close to the pulmonary and aortic valves. Usually they have LBBB-like shape. Outflow tract VPBs (right ventricular outflow tract [RVOT] and left ventricular outflow tract [LVOT]) are the most common variety of “benign” VPBs occurring in a normal heart. VPBs originating closer to the apex and from inferior wall activate the heart from the bottom up and are said to have “superior” axis, with QRS negative in leads II, III, and aVF. VPBs originating in the area of postinfarct myocardial scar often have a qR configuration. Sometimes this allows diagnosing infarct even when no Q waves are seen during sinus rhythm (see Fig. 16-7).
The sequence of ventricular repolarization after VPBs is such that ST-T waves are directed in the opposite direction to the main QRS deflection (QRS-T “discordance”), often with prominent ST segment elevations/depressions as expected (see Fig. 16-2). Clinicians need to recognize that these secondary ST-T changes are not due to ischemia and are similar to the QRS-T discordance findings in wide complex beats due to bundle branch block and ventricular pacing. In fact, concordance between QRS and ST-T directions during VPBs may be a sign of myocardial injury.
Coupling Interval
The term coupling interval refers to the interval between the VPB and the QRS of the preceding normal beat. When multiple VPBs are present, fixed coupling often occurs, with the coupling interval approximately the same for each VPB (see Fig. 16-6). At other times, VPBs may show a variable coupling interval. Whether VPBs demonstrate fixed versus variable coupling does not have major clinical implications.
Compensatory Pauses
As you may have noticed, APBs and VPBs are usually followed by a pause before the next normal sinus beat. The pause after a VPB is usually but not always longer than the pause after an APB. A fully compensatory pause indicates that the interval between the normally sinus-generated QRS complexes immediately before and immediately after the VPB is twice the basic PP interval (Figs. 16-8 and 16-9). A fully compensatory pause is more characteristic of VPBs than APBs. The explanation for this difference (see Fig 16-9) relates to the fact that PVCs usually do not reset (delay) firing of the sinus node, although supraventricular beats often do.