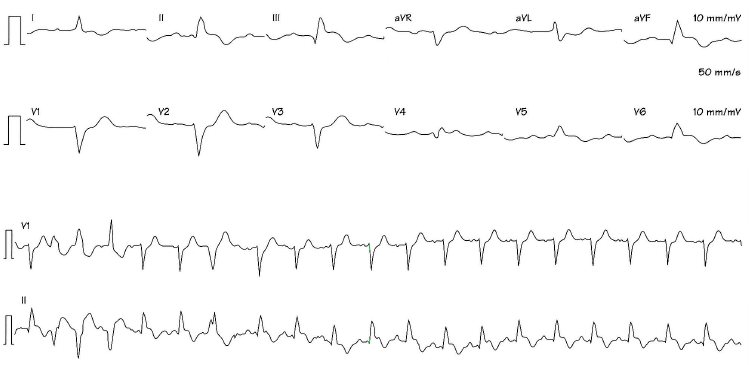
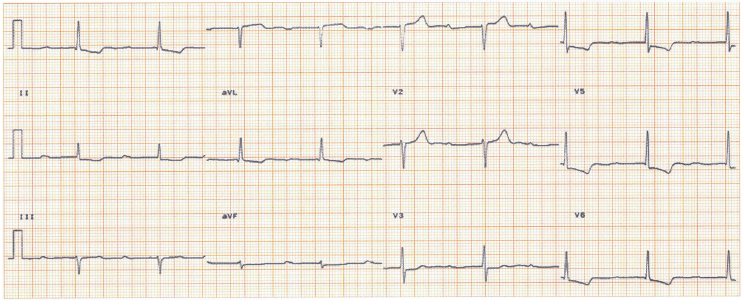
Your opinion is requested on the pre-operative risk assessment of a moderately obese 79-year-old female due to undergo hip replacement surgery. She has treated hypertension, no prior cardiac illness, can walk a hundred yards before stopping with hip discomfort. Exam shows sinus rhythm, rate 80, blood pressure 138/82, no signs of heart failure, no murmers. Figure 1 shows her ECG.
1What does it show and does it help pre-operative risk assessment?
What, if any, further investigations are appropriate?
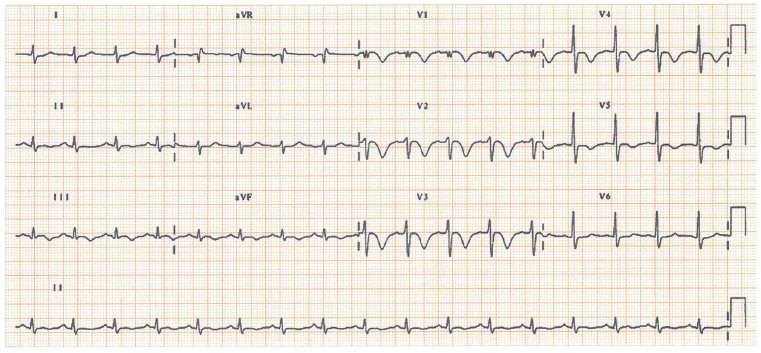
She undergoes successful hip replacement surgery. Eight months later she presents acutely with severe chest pain. radiating down both arms, with associated sweating. Exam shows her to be in pain, otherwise unremarkable.
2What does the ECG (Fig. 2) show, and how should she be treated?
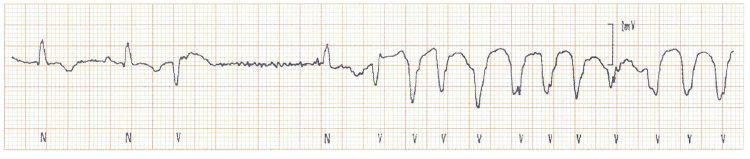
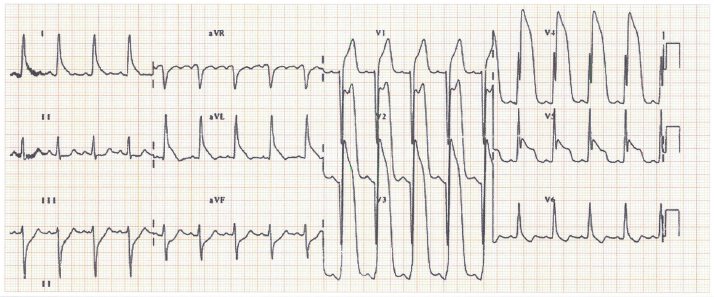
Two days after admission, she develops fast regular palpitations, with a blood pressure of 85/55. This ECG (Fig. 3) records the onset of her arrhythmia.
3 What does it show, and what is the mechanism for her arrhythmia?
1 The only abnormality is rather small QRS complexes; this could reflect myocyte loss, but a cardiac ultrasound was normal, the R waves therefore relate to her obesity, and the ECG was normal. Operative risk depends on the nature of the planned surgery, and seven risk factors (age > 70 years, current angina, previous myocardial infarction, chronic heart failure, prior cerebrovascular event, diabetes mellitus and chronic renal failure). The resting ECG does not, in most cases, add data beyond these variables. No further evaluation is required, and the patient underwent uneventful surgery.
2 The ECG is taken at standard sensitivity (10 mm/mV) but twice normal speed (50 mm/s), accounting for the apparent QRS broadening. Sinus rhythm, normal P wave, PR interval, ST elevation II. III, aVF, V4–6. The diagnosis is an infero-lateral ST segment elevation myocardial infarction (STEMI). Thrombolysis or primary percutaneous coronary intervention (PCI) is the treatment. The rhythm strip shows ventricular ectopics of different shapes initially, then sinus rhythm.
3 The strip starts with two supraventricular beats (the second one clearly sinus, with a preceding P wave, the first of less certain aetiology). There is then a ventricular ectopic, and a considerable pause, followed by one sinus beat, then a run of a broad complex tachycardia, clearly ventricular tachycardia. The mechanism of the ventricular tachycardia (VT) is pause-dependent QT lengthening. The VT was sustained and required DC cardioversion.
See Chapter 50 for further details.
Case 2
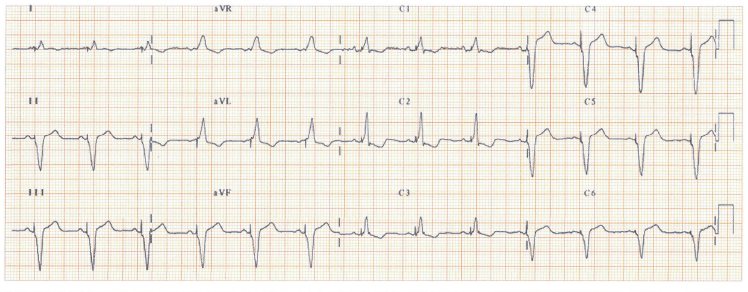
1 Regular unremarkable P waves. Broad QRS complex, preceded by a pacing spike (best seen in leads V3–6). This is a ventricular paced rhythm; as there is a P waves before each QRS complex, this is a dual chamber pacemaker, tracking the atria, pacing the ventricle. The QRS is dominant (i.e. large R wave) in lead VI giving the appearance of right bundle branch block, due to late right ventricle activation. ‘Normal’ ventricular pacing activates the right ventricle first, then the left ventricle (as the pacing wire is sited in the right ventricle apex), giving an appearance similar to left bundle branch block. The pattern here indicates that the left ventricle (LV) is activated first, either as the ventricular pacing wire has been placed by mistake in the LV (i.e. going from the superior vena cava/right atrium, via a patent foramen ovale, into the left atrium and ventricle) or, much more likely, if the patient has a multisite ventricular pacemaker pacing the LV free wall, resynchronizing dyscoordinate LV contraction.
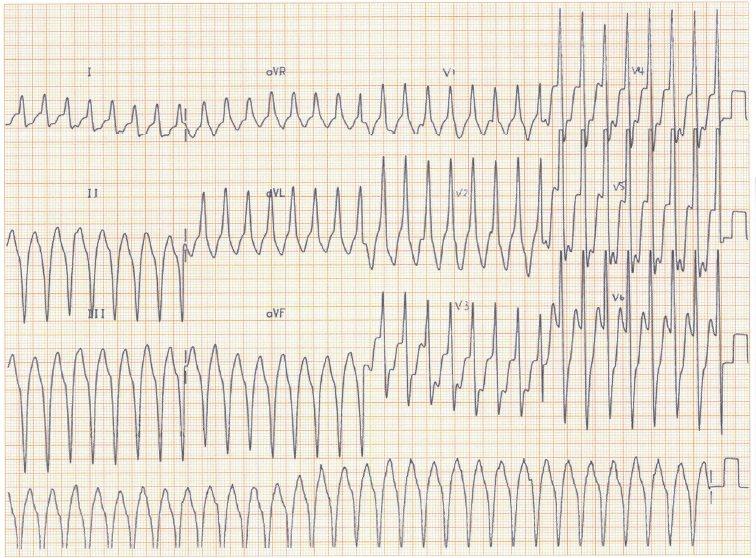
A 67-year-old man with a remote myocardial infarction develops fast regular palpitations, with light-headedness. In hospital he is fully conscious, has slightly cool skin, O2 saturation 97% on air, heart rate 160 b/min, blood pressure 85/50, venous pressure raised, no pedal oedema, an irregular variation in the first heart sound.
1What does the ECG show (Fig. 5) and what is the treatment?
An 85-year-old hypertensive man, presents with a blackout. While standing in the kitchen, without warning, he fell to the ground, unconscious. He was described as ‘looking dead’. Moments later he recovered fully. Examination shows bilateral black eyes, normal cardiovascular exam. His ECG is shown in Fig. 6.
A 35-year-old man returns from a holiday in Greece, presents with brief syncope, followed by intermittent breathlessness and anxiety. He looks pale, O2 Saturation 93% on air, heart rate 120 b/min, blood pressure 90/55, venous pressure + 6 cm, loud first heart sound, no murmurs, clear chest.
1What does the ECG (Fig. 7) show? What should be done?
1 This ECG shows ventricular tachycardia (VT). Why? There is a broad complex tachycardia; an experienced observer will instantly recognize VT. Ninety per cent of broad complex tachycardias in those with previous myocardial infarction (MI) are VT, so chance alone says this is VT. In supraventricular tachycardia with aberrancy, the complexes look like right or left bundle branch block (RBBB or LBBB), not the case here. With its dominant R wave in lead VI, this appears most like RBBB, but in fact doesn’t look at all like the staggered M of typical RBBB. The straight up-down pattern is highly suggestive of VT. What clinches the diagnosis is the independent (i.e. varying relationship to each QRS complex) atrial activity seen in leads II and VI as occasional irregularities in the baseline. The right-bundle pattern – superior axis (+ve QRS in lead I, –ve in II, III) suggests the VT originates in the inferior wall of the left ventricle. Though with only mild haemodynamic compromise, one could try intravenous drugs; DC cardioversion under general anaesthesia is a safe reliable treatment. In the longer run, exclusion of another MI, assessment of left ventricular function and coronary anatomy are needed, and probably revascularization and implantable cardioverter defibrillator (ICD) implantation.
See Chapter 49 for further details.
Case 4
1 The P wave is broad (lead II), suggesting left atrial enlargement. The PR interval is 520 ms (normal < 200 ms). The QRS duration and axis are normal. The R waves are unremarkable. The lateral T waves are inverted. The interpretation is: (a) extensive conducting system disease of the AV node or, more likely, the infra-Hissian system, causing an episode of complete heart block and so a Stokes–Adams attack; (b) lateral lead T waves changes could reflect ishaemic heart disease as the T waves changes spread to lead V3, or, despite the normal R waves, hypertensive heart disease (not aortic stenosis, as no murmer) – left ventricular hypertrophy with unremarkable R waves is not rare in the elderly. Digoxin causes a long PR interval (rarely this long) and lateral T changes. Provided there is no acute coronary syndrome, the right treatment is a permanent pacemaker.
See Chapter 55 for further details.
Case 5
1 Sinus tachycardia, 103 b/min, normal P waves, PR interval. QRS axis shifted to the right (+ 107°), impressive T wave inversion septally (V1→3). and more laterally, mildly so inferiorly. The differential diagnosis includes an acute coronary syndrome (ACS) (and myocarditis), but the sinus tachycardia, right axis QRS deviation and V1→3 T wave inversion are together so highly suggestive of a large pulmonary embolism as to be almost diagnostic. A cardiac ultrasound will support the diagnosis (and decrease that of an ACS). A computed tomography (CT) pulmonary angiogram will confirm the diagnosis. Intravenous heparin/thrombolytic therapy may be required.