Table 15.1 Types of Prosthetic Valvesa | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
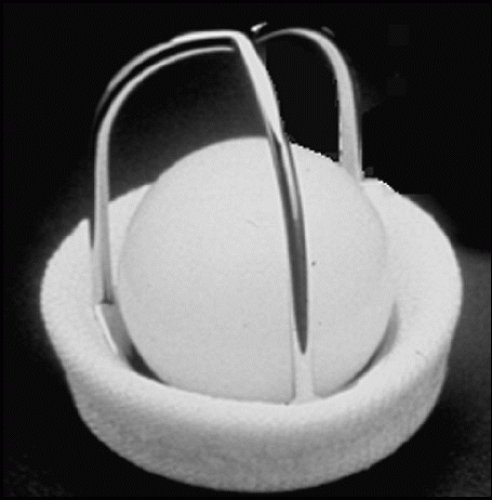 FIGURE 15.1. A Starr-Edwards prosthesis. |
 FIGURE 15.2. A St. Jude prosthetic valve. |
 FIGURE 15.3. A porcine bioprosthetic valve. |
prosthetic valves often requires a combination of transthoracic and transesophageal imaging. Although the role of threedimensional imaging continues to evolve, the improved spatial orientation provided by modern equipment provides a unique and potentially valuable perspective. Two-dimensional echocardiography is used to determine the type of valve and to evaluate its structure and function. Using this modality, the stability of the sewing ring is assessed. Rocking or independent motion of the prosthesis is often an indication of dehiscence. The presence of abnormal masses, such as thrombi or vegetations, should be determined. Shadowing from the prosthesis may obscure such pathology and multiple imaging windows may be required for a complete evaluation. Motion of the leaflets, disks, or occluder mechanism should also be assessed from the two-dimensional study. An important early step in the echocardiographic assessment of prosthetic valves is recognizing the range of normal findings. Figure 15.4 is a normally functioning porcine aortic prosthesis. Leaflet opening during systole resembles that of a normal native valve. The overall appearance is so similar, in fact, that normally functioning aortic bioprostheses are occasionally mistaken for “normal” aortic valves when historical information is not available. When examined carefully, however, the sewing ring and struts are more echogenic than normal and tend to shadow the leaflets, a clue to the presence of prosthetic material. A normal porcine mitral prosthesis, assessed using three-dimensional echocardiography, is shown in Figure 15.5. Note how this technique permits the valve to be visualized from opposite perspectives, the left atrial side and the ventricular aspect.
Table 15.2 Indications for Echocardiography in Interventions for Valvular Heart Disease and Prosthetic Valves | ||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||
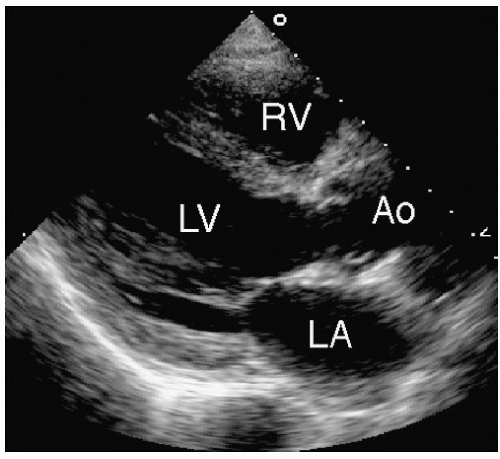 FIGURE 15.4. An echocardiogram of a normally functioning porcine bioprosthetic aortic valve. |
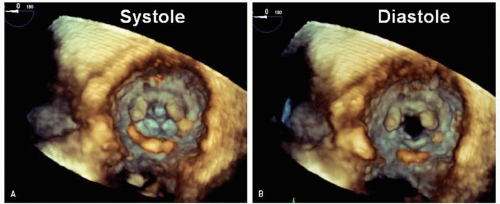 FIGURE 15.5. A three-dimensional echocardiogram of a normal porcine mitral prosthesis is shown in systole (A) and diastole (B). This view is taken from the left ventricular perspective and shows the struts pointing into the left ventricle. A view from the opposite side, the left atrium, is also possible. |
a higher resistance to forward flow compared with equivalently sized native valves. Thus, flow velocity through a normally functioning artificial valve is generally higher than would occur through a normal native valve. However, the range of velocities through a normally functioning bioprosthesis is considerable. Both valve size and type determine the pressure gradient that one can expect in the absence of dysfunction. For example, stented bioprosthetic valves may have slightly higher gradients than mechanical valves of similar size, which tend to have higher gradients than stentless valves. For all these reasons, the range of velocities that must be considered normal varies widely among prosthetic valves. This is illustrated in Figure 15.11. In Figure 15.11A, a newly implanted St. Jude aortic prosthesis is shown. Although functioning normally by clinical criteria, the Doppler study demonstrates a maximal velocity of 290 cm/sec and a mean gradient of 20 mmHg. Also note the distinctive “clicks” that correspond to the opening and closing of the disks. In contrast, Figure 15.11B illustrates flow through a normally functioning bioprosthetic aortic valve. In this case, no significant increase in velocity is present. Prosthetic valve clicks are not typically seen in normally functioning bioprostheses.
 FIGURE 15.6. A normally functioning Starr-Edwards mitral prosthesis. A: During systole, the poppet is seated within the sewing ring (arrows). B: During diastole, the poppet moves forward into the cage (arrows), allowing blood flow around the occluder. |
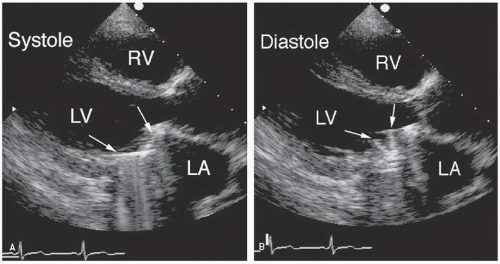 FIGURE 15.7. A normally functioning St. Jude mitral prosthesis. A: During systole, the hemidisks are shown in the closed position (arrows). B: During diastole, the two disks are recorded in the open position (arrows). |
overestimation of true gradient occurs. Flow through a caged ball valve does not go through a well-defined orifice but rather goes around the periphery of the spherical occluder (Fig. 15.13). The variability and orientation of the flow complicate the Doppler interrogation of these valves. Flow through bioprostheses is often triangular in shape and may occur through an area that is significantly smaller than the sewing ring itself. Note in Figure 15.14 the position of the three struts and how they effectively form a triangular orifice, the area of which is considerably smaller than the surrounding sewing ring. All these factors contribute to the challenges inherent to assessing prosthetic valve function by any technique.
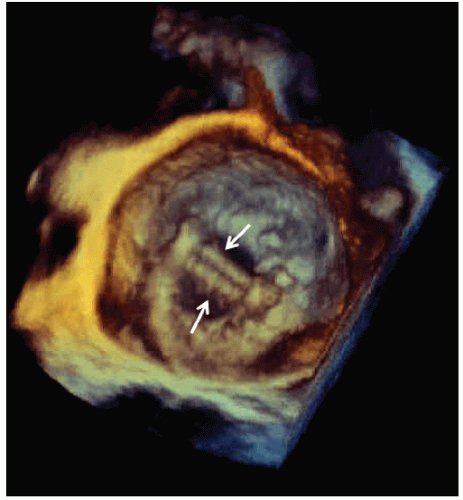 FIGURE 15.8. A three-dimensional echocardiogram of a normal St. Jude mitral prosthesis is shown from the perspective of the left atrium. In real time, the hemidisks (arrows) are seen to open and close from above. |
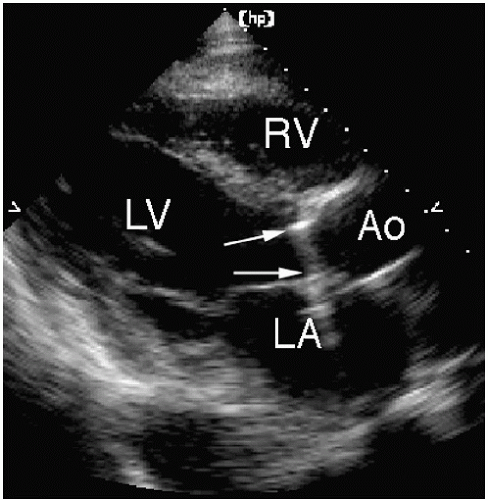 FIGURE 15.9. A normally functioning St. Jude aortic prosthesis. The sewing ring is indicated by the arrows. The walls of the aortic root often obscure the motion of the disks. |
as pressure recovers (or increases) downstream, the net pressure gradient diminishes. This means that Doppler imaging, by recording the maximal velocity within the vena contracta, will demonstrate a higher gradient compared to catheter-based methods, which will be lower due to pressure recovery. Although pressure recovery is one potential explanation for a discrepancy in which Doppler imaging reports a higher gradient than catheterization, it does not imply that either method is “right” or “wrong”, rather that local changes in pressure will naturally result in differences in methodology. It should be emphasized that this higher gradient value obtained by Doppler imaging is a real phenomenon, although less physiologically relevant than the net gradient between the left ventricle and the aorta. This concept of pressure recovery is further discussed in Chapter 9.
 FIGURE 15.10. A normally functioning Medtronic Freestyle valve is shown in the aortic position. A: During systole, the valve is shown in the opened position. B: During diastole, the cusps are barely visible. Normally functioning stentless valves appear very similar to normal native valves. |
 FIGURE 15.11. Doppler evaluations of a normally functioning St. Jude bileaflet prosthesis (A) and a porcine prosthesis (B). In both cases, contour of the flow signal and maximal velocity are within the expected range. Note the opening and closing valve clicks that are associated with the mechanical but not the tissue prosthesis. AV, aortic valve. |
 FIGURE 15.12. A transesophageal echocardiogram from a patient with a St. Jude mitral prosthesis demonstrates the appearance of the discs during diastole (A) and systole (B). This technique is ideal to record opening and closing of the hemidisks. C: Flow through one of the larger semicircular orifices is recorded using transthoracic Doppler imaging. |
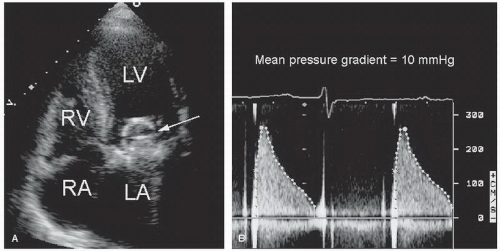 FIGURE 15.13. A: A Starr-Edwards mitral prosthesis (arrow). B: Doppler imaging demonstrates flow through the valve. The mean pressure gradient is approximately 10 mm Hg. |
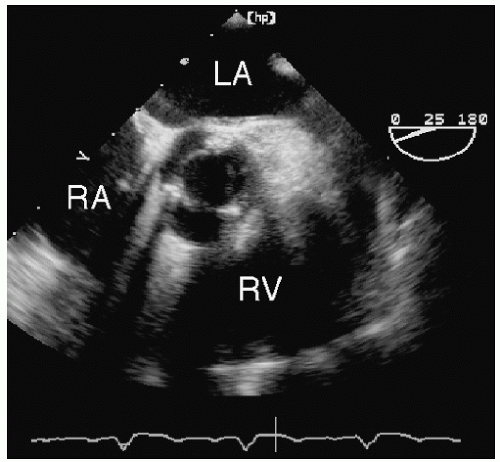 FIGURE 15.14. A short-axis view of a porcine aortic prosthesis from transesophageal echocardiography. The three struts are visualized, forming a triangular-shaped orifice. |
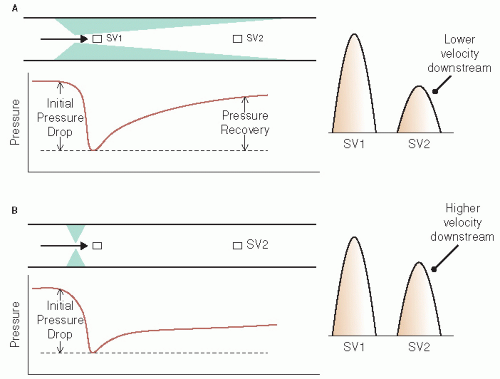 FIGURE 15.15. The concept of pressure recovery. A: In the absence of pressure recovery, different locations for sample volume (SV) measurement yield fairly similar velocities. B: Flow through a tapered stenosis results in significant pressure recovery downstream from the obstruction. In this case, sampling within the obstruction (SV1) yields a higher velocity compared with a sample site downstream (SV2) where pressure recovery has occurred. At this site, the recovery of pressure is associated with a lower velocity. See text for details. |
imaging study in all patients at a time when the valve is known to be functioning normally, such as during the first postoperative clinic visit. This can then be used as a reference for future evaluations to help determine whether a given pressure gradient is normal or abnormal for the individual. In addition, tables have been published providing a range of normal values for different types of valves in the various positions.
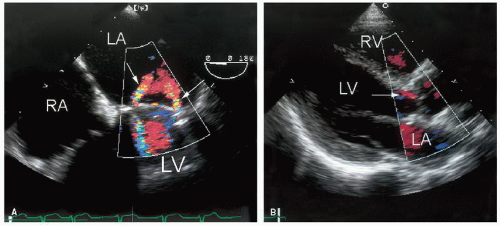 FIGURE 15.16. Physiologic regurgitation through a normally functioning St. Jude mitral prosthesis (arrows) (A) and a porcine aortic prosthesis (arrow) (B). |
 FIGURE 15.17. Physiologic regurgitation through a St. Jude aortic valve. The jets originate at the periphery and appear to cross just below the valve (arrow). The occurrence of this type of regurgitation is part of the design of many prosthetic valves. |
not performed previously, is essential for optimal intraoperative management. Thus, echocardiography is routinely used prior to valve surgery (to make decisions regarding type and size of prosthesis, feasibility of repair, etc), during surgery (to assess the success and completeness of the procedure), and following surgery (to establish a new baseline and to document a successful procedure). The specific indications for intraoperative transesophageal echocardiography are listed in Table 15.3. Its value in this setting is well documented. Clinical series indicate that intraoperative echo results change the operative plan in up to 15% of cases and identify a problem of sufficient magnitude to warrant revision in approximately 5% of patients. This is especially true in valve surgery, particularly valve repair procedures. As expected, the potential value of echocardiography is directly related to the complexity of the procedure. Valve repair, replacement of multiple valves, valve surgery involving complicated endocarditis, and valve replacement involving stentless valves or homografts are examples of technically challenging operative procedures where to value of intraoperative echocardiography is well established.
 FIGURE 15.18. Doppler imaging is used to record flow through an aortic prosthesis. The peak and mean gradients are indicated. Note the presence of valve clicks at the time of opening and closing. |
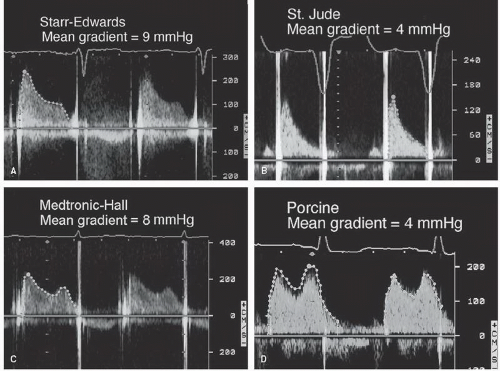 FIGURE 15.19. A-D: Doppler recording of flow through four different mitral prosthetic valves. The mean gradient across each prosthesis is indicated. |
Table 15.3 Intraoperative Assessment Using Transesophageal Echocardiography | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||
of dysfunction. Both American College of Cardiology/American Heart Association Management Guidelines and Appropriateness Criteria have been published to provide guidance in this area (see Table 15.4). From these documents, there is general consensus that echocardiography should be performed soon after valve surgery as part of the initial evaluation of the patient during the recovery phase. This examination should focus on an assessment of left and right ventricular function, determination of pulmonary artery pressure, and, of course, a thorough evaluation of the repaired or replaced valve. Because all prosthetic valves have some degree of obstruction, a critical part of the evaluation is to determine the pressure gradient. Careful assessment of regurgitation is also important. Mild valvular regurgitation is normally present in many prosthetic valves. On the other hand, perivalvular regurgitation is usually an abnormal finding that requires thorough assessment and follow-up. Thus, the initial postoperative echocardiogram should clearly document the presence and severity of regurgitation and differentiate normal from abnormal forms.
Table 15.4 Evidence-based Indications and Appropriateness Criteria Related to the Evaluation of Prosthetic Valves | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
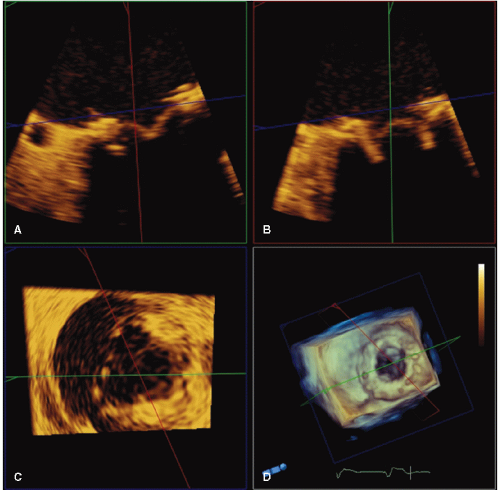 FIGURE 15.20. A porcine mitral prosthesis is evaluated with transesophageal three-dimensional echocardiography. Panels A and B are systolic frames of the prosthesis with two-dimensional echocardiography. Panel C is a short-axis view of the prosthesis. In panel D, a volume rendered three-dimensional image provides a clear circumferential view of the sewing ring. |
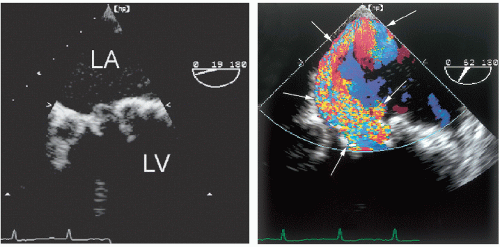 FIGURE 15.21. An example of primary tissue degeneration involving a porcine mitral valve. The leaflets are thickened and fibrotic with decreased mobility (left). Right: Color Doppler imaging demonstrates severe mitral regurgitation with an eccentric jet (arrows). |
 FIGURE 15.22. A: An example of a mildly thickened porcine mitral prosthesis. The structure and motion of the leaflets are often obscured by the struts. B: Doppler imaging demonstrates a mean gradient of 10 mmHg. MV, mitral valve. |
 FIGURE 15.23. M-mode echocardiogram of a St. Jude mitral prosthetic valve. M-mode echocardiography is ideal to record the brisk opening and closing of the disks (arrows). IVS, interventricular septum; MV, mitral valve. |
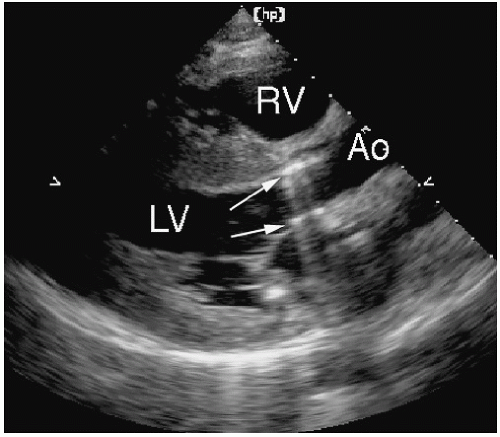 FIGURE 15.24. The presence of a St. Jude aortic prosthesis (arrows) creates a pattern of reverberations that extends into the left atrium. This creates a shadowing effect and can obscure the presence of mitral regurgitation. |
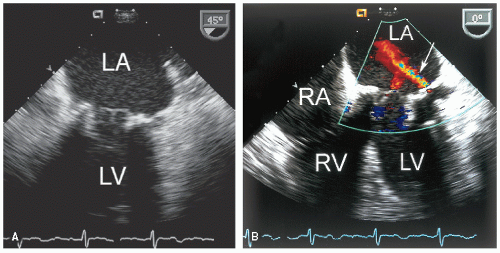 FIGURE 15.25. A: A porcine mitral prosthesis is visualized using transesophageal echocardiography. B: Color Doppler imaging demonstrates both transvalvular and perivalvular (arrow) mitral regurgitation. |
time (Fig. 15.26). Three-dimensional transesophageal imaging will likely prove to be the most sensitive method for this determination. Figure 15.27 is an example of flow through a normally functioning mechanical mitral prosthesis recorded with real-time three-dimensional imaging. In this example, both antegrade flow and mild regurgitant flow are demonstrated. One advantage of this approach is the ability to distinguish flow through the various orifices of a mechanical prosthesis. Spectral Doppler recordings of prosthetic valve flow will also include brief, high-velocity signals referred to as “clicks.” These are intense recordings associated with both the opening and closing of the occluder mechanism. They provide useful information on timing and are particularly helpful to identify the various phases of filling and ejection. In Figure 15.28, both normal and abnormal St. Jude aortic prostheses are shown. In Figure 15.28A, note the valve clicks marking opening and closing of the normal valve. Figure 15.28B is taken from a patient with a prosthesis that is partially obstructed by a thrombus on the sewing ring. Note that the opening valve click is absent, and the closing click is very faint. The high velocity is evidence of the increased pressure gradient across the partially obstructed valve.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


