a very small amount of fluid in the pericardial space that typically collects in the dependent areas. It is most often appreciated as a very small echo-free space in the posterior atrioventricular groove. This space may increase in size during systole (Fig. 10.1). In the absence of a pericardial effusion, dramatic thickening, or calcification, it is unusual to directly visualize the pericardium with either M-mode or two-dimensional echocardiography. Intracardiac ultrasound has been used to directly visualize the pericardium but is infrequently used for this purpose in clinical practice.
Table 10.1 Etiology of Pericardial Disease | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 10.2 Appropriateness Criteria for Use of Echocardiography in Known or Suspected Pericardial Disease | |||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||
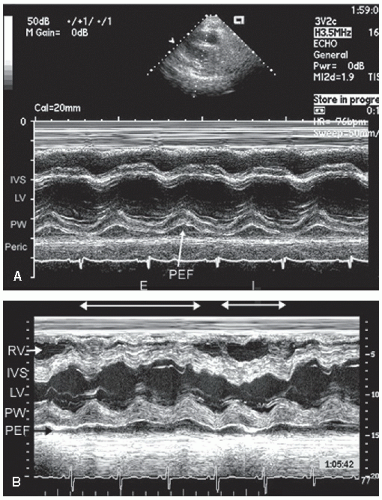 FIGURE 10.1. M-mode echocardiograms recorded in patients with pericardial effusions. A: Note the echo-free space (arrow) immediately behind the posterior wall of the left ventricle consistent with a small pericardial effusion (PEF). Also note that the space is larger in systole than in diastole. B: The patient has a larger pericardial effusion with respiratory variation in right ventricular size and septal position. |
represents the normal amount of pericardial fluid in a disease-free state (Fig. 10.2). It is visualized as a small echo-free space in the posterior atrioventricular groove that may be visible only in systole when the heart has pulled away from the pericardium. A small effusion is defined as one resulting in as much as 1 cm of posterior echo-free space, with or without fluid accumulation elsewhere. Smaller effusions tend to collect in the dependent aspect of the pericardial space and, as such, their exact position may vary with patient position. Moderate effusions have been described as 1 to 2 cm of echo-free space and large effusions as more than 2 cm of maximal separation. It should be emphasized that these definitions may vary from laboratory to laboratory. In large effusions, the heart may swing within the pericardial space (Figs. 10.7 and 10.10).
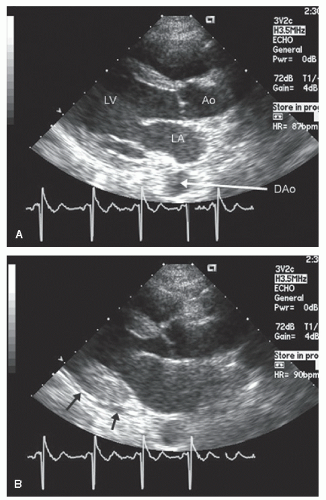 FIGURE 10.2. Parasternal long-axis echocardiogram recorded in a patient with a minimal pericardial effusion. This amount of pericardial fluid represents the normal fluid seen in disease-free individuals. A: Recorded at end-diastole. B: Recorded at end-systole. Note that at end-diastole, there is no separation between the epicardium and the pericardium. At end-systole, the epicardium has lifted off the pericardium revealing a very small pericardial effusion, maximal in the posterior interventricular groove (arrows). DAo, descending aorta. |
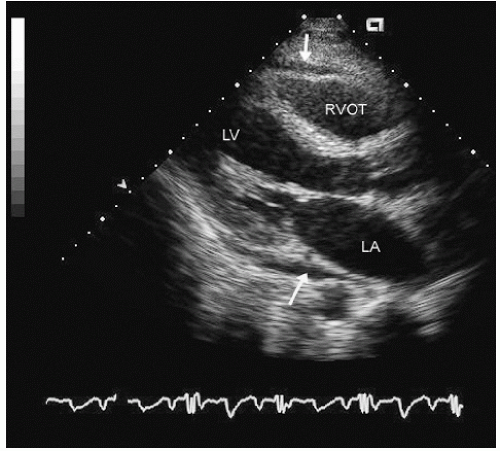 FIGURE 10.3. Parasternal long-axis echocardiogram recorded in a patient with a small pericardial effusion. Note the echo-free space, maximal in the posterior interventricular groove (arrow) and a smaller anterior echo-free space (downward-pointing arrow). In the real-time image, this pericardial effusion can be seen to be present both in diastole and in systole. |
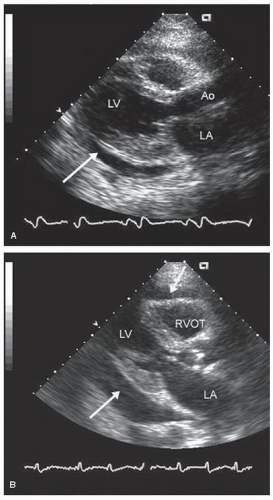 FIGURE 10.4. Parasternal long-axis echocardiograms recorded in patients with a small (A) and moderate to large (B) pericardial effusion. A: There is an approximately 1-cm space between the epicardium and the pericardium (arrow), consistent with a small pericardial effusion. B: A larger pericardial effusion is present both anteriorly and posteriorly (arrows). |
pericardial fluid volume and distribution but is limited in its availability. Using this technique, the three-dimensional volume of the entire pericardial space can be calculated. The overall total volume of the entire heart (all four chambers) is then likewise calculated, and the pericardial fluid volume is calculated as the difference between these two volumes. Three-dimensional echocardiography may be limited for this purpose because of a limited field of view, which may preclude registration of a three-dimensional data set of significant size to encompass the entire pericardial volume in larger effusions. Although probably accurate for determining the volume of pericardial fluid, this technique has had little clinical acceptance because of the limited availability of three-dimensional scanning and the lack of a clinical need for determining precise pericardial volume as opposed to its hemodynamic effect.
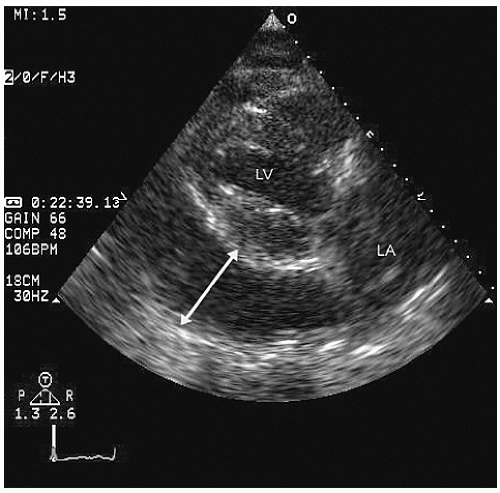 FIGURE 10.5. Parasternal long-axis echocardiogram recorded in a patient with a large pericardial effusion, measuring 4 cm in its greatest dimension posteriorly (arrow). In the real-time image, there is evidence of a swinging heart. |
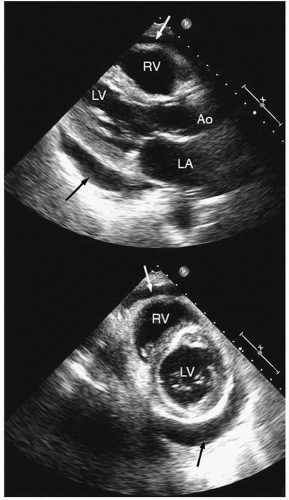 FIGURE 10.6. Parasternal long- and short-axis views of the heart in a patient with a circumferential small to moderate pericardial effusion (arrows). Note the effusion posterior to the left ventricle and anterior to the right ventricle and a mobility of the heart within the pericardial space in the real-time image. |
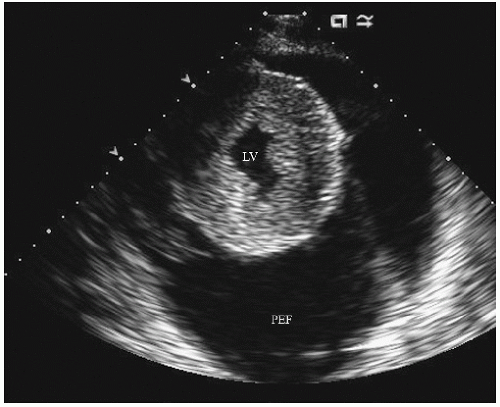 FIGURE 10.7. Parasternal short-axis view recorded in a patient with a massive pericardial effusion (2,500 mL drained at the time of pericardiocentesis). Note the free motion of the heart within the pericardial space. Also note the marked left ventricular hypertrophy secondary to hypertensive heart disease. PEF, pericardial effusion. |
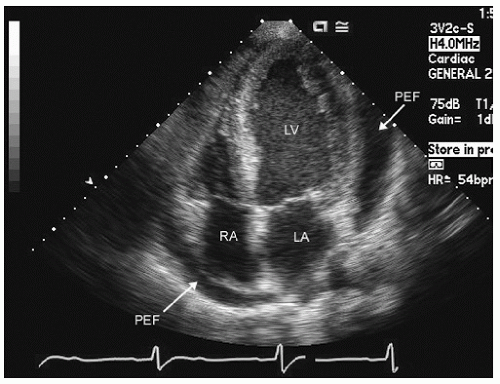 FIGURE 10.8. Apical four-chamber view recorded in a patient with a moderate, predominantly lateral pericardial effusion (PEF) (arrow). Also note a smaller fluid collection behind the right atrium. |
 FIGURE 10.9. Subcostal echocardiogram reveals a moderate to large pericardial effusion. Note the effusion surrounding the entire heart, with its greatest dimension lateral to the left ventricular free wall. Fluid is clearly seen surrounding the right atrium and between the pericardium and the right ventricle. |
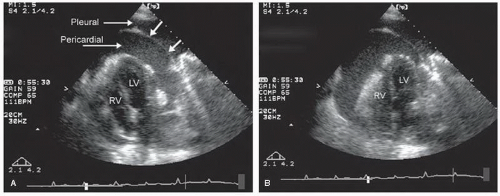 FIGURE 10.10. Apical four-chamber view recorded from a patient with a large pericardial effusion and a swinging heart. A pleural effusion is also present, which allows direct visualization of the pericardial thickness (arrows) (A). A, B: Recorded from different cardiac cycles. Note the marked change in position of the heart within the pericardial space, which can be appreciated as a swinging heart in the real-time image. This variable position within the thorax is the cause of electrical alternans seen on surface electrocardiography. |
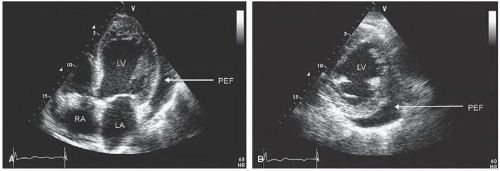 FIGURE 10.11. Apical four-chamber (A) and parasternal short-axis (B) views recorded in a patient with a small, localized, predominantly lateral pericardial effusion (PEF). This echocardiogram was recorded approximately 2 weeks after open-heart surgery. |
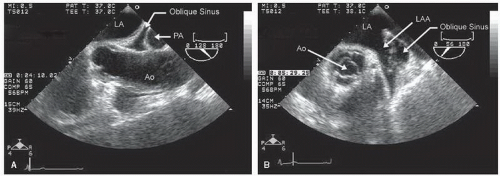 FIGURE 10.12. Transesophageal echocardiogram recorded in a patient with a moderate pericardial effusion and evidence of fluid in the oblique sinus. A: Note the echo-free space bounded by the left atrium, aorta, and pulmonary artery (PA). This represents fluid accumulating in the pericardial reflection around the great vessels. B: There is a similar collection of fluid in the pericardial space surrounding the left atrial appendage (LAA). In the real-time image (B), note the excessive motion of the wall of the left atrial appendage within the pericardial fluid in the oblique sinus. On occasion, the wall of the left atrial appendage can assume a masslike appearance and be confused with a pathologic mass. |
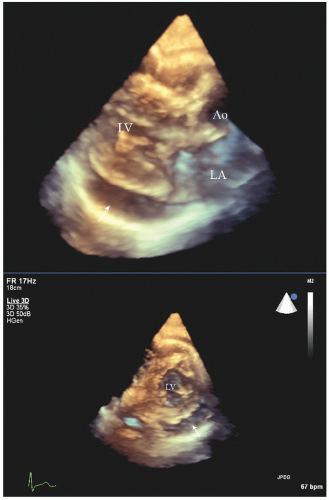 FIGURE 10.13. Transthoracic real-time three-dimensional imaging in a patient with a moderate pericardial effusion in parasternal long- and short-axis views. Note the circumferential effusion surrounding the left and right ventricles (arrows) and the excellent visualization of the extent of free fluid surrounding the heart. |
calcific pericarditis, there may be marked shadowing seen posterior to the pericardium (Fig. 10.15). It should be emphasized that the normal pericardium is a highly reflective structure and that a bright pericardial echo alone should not be used to establish the diagnosis of constrictive pericarditis or of a thickened pericardium.
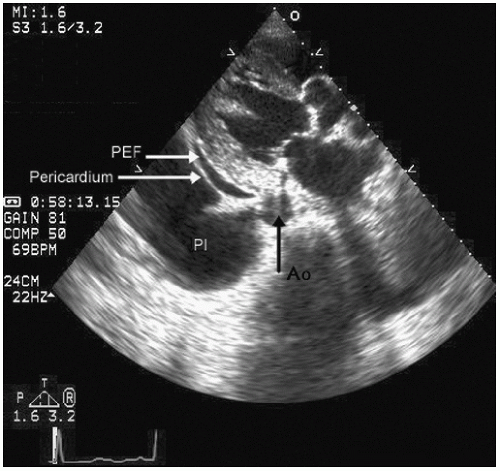 FIGURE 10.14. Parasternal long-axis echocardiogram recorded in a patient with a small pericardial effusion (PEF) and a larger pleural effusion (Pl). The presence of concurrent pericardial and pleural fluid allows identification of the parietal pericardium. In this instance, the pericardial thickness can be seen to be approximately 2 mm. Note the position of the two fluid collections with respect to the descending thoracic aorta (black arrow). |
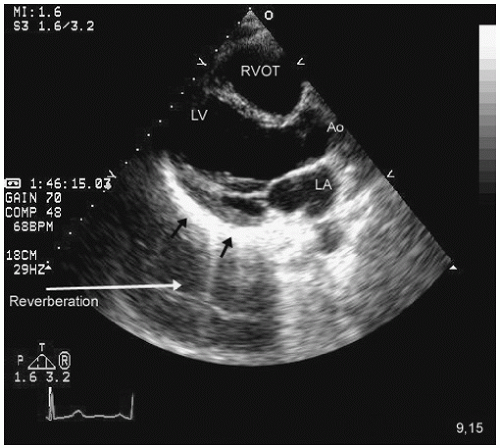 FIGURE 10.15. Parasternal long-axis echocardiogram recorded in a patient with a partially calcified posterior pericardium (arrows). The posterior pericardium has pathologic echo intensity and appears thickened, although because of reverberation, the actual thickness cannot be reliably determined. The markedly echogenic pericardium has resulted in reverberation artifact, creating a double image of the left ventricular cavity behind the pericardial space, best appreciated in the real-time image. |
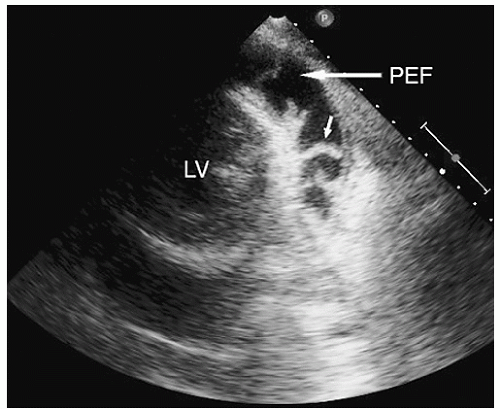 FIGURE 10.16. Parasternal short-axis view recorded in a patient with a moderate pericardial effusion related to uremic pericarditis. Note the multiple fibrous strains (arrow) in the pericardial space, many of which appear to bridge the parietal and visceral pericardia. |
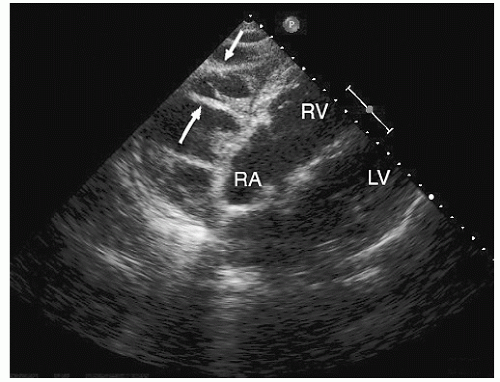 FIGURE 10.17. Subcostal imaging recorded in a patient with a moderate to large loculated effusion predominantly located over the right atrium and right ventricle related to prior cardiac surgery. As in Figure 10.16, note the inflammatory stranding bridging between the visceral and the parietal pericardia and the appearance of multiple loculated fluid collections. |
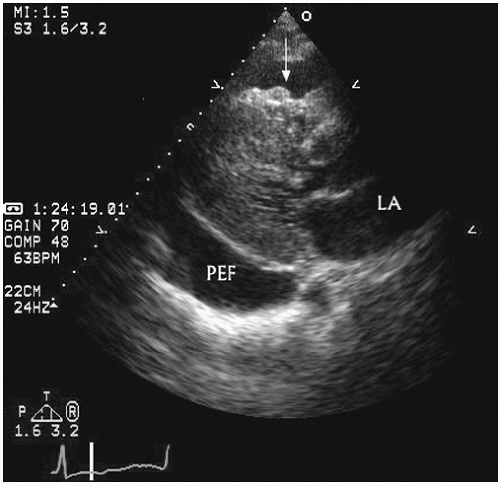 FIGURE 10.18. Parasternal long-axis echocardiogram recorded in a patient with a large malignant pericardial effusion (PEF). Note the nodular densities overlying on the visceral aspect of the pericardium anteriorly (arrow). Of note, similar densities may be seen in nonmalignant processes as well. |
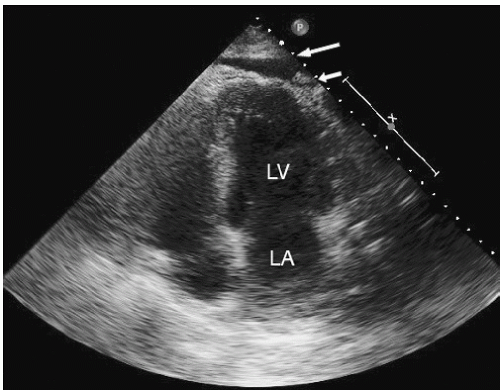 FIGURE 10.19. Apical four-chamber view recorded in a patient with an inflammatory pericardial effusion related to connective tissue disease. Note the free fluid in the pericardial space overlying the apical and lateral wall of the left ventricle (longer arrow) and the nodular density adherent to the visceral pericardium (smaller arrow) which, in this case, was not associated with malignancy. |
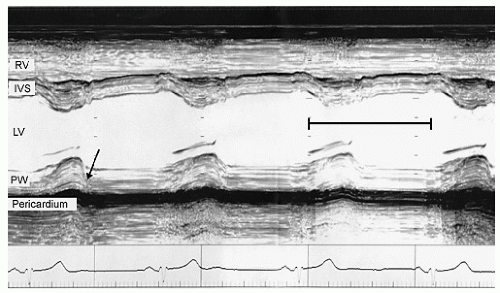 FIGURE 10.20. M-mode echocardiogram recorded in a patient with constrictive pericarditis and thickened posterior pericardial echoes. To the right of this frame, in the area marked by the black bracket, damping has been increased to suppress the fainter myocardial echoes. Note that the bright pericardial echo has not been suppressed. Also note the flat motion of the posterior wall after the initial rapid posterior motion (arrow) of the endocardium. PW, posterior wall. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


