The ductus arteriosus is a vascular communication between the systemic and pulmonary vasculature, usually between the isthmus of the aortic arch and the origin of the left pulmonary artery, which forms a vital part of the fetal vascular anatomy. Normally, the ductus arteriosus arises from persistence of the distal portion of the embryonic sixth aortic arch.
FETAL CIRCULATION
In the fetus, the lungs are not ventilated and pulmonary resistance is high. The majority of relatively desaturated venous blood from the superior vena cava returning to the right ventricle passes through the ductus arteriosus into the descending aorta, whence some of it exits the fetal body through the umbilical artery to be oxygenated by the placenta. The ductus arteriosus is normally strategically positioned so that this desaturated blood does not travel to organs with the greatest oxygen metabolism (the brain and myocardium). After birth, pulmonary gas exchange commences and the circulation is “in series.” With the ductus arteriosus no longer essential, spontaneous closure normally occurs in hours to a few days after birth.
MECHANISMS OF SPONTANEOUS DUCTAL CLOSURE
Ductal closure occurs in two stages. The first is functional closure, occurring within the first 6 to 15 hours after birth. This stage results from medial smooth muscle constriction, promoted by four principal factors: (1) increase in arterial oxygen tension, (2) decrease in circulating prostaglandin E2 (PGE2), (3) decrease in mean ductal blood pressure, and (4) decline in the density of PGE2 receptors in the ductal wall. Part of the oxygen dependence is intrinsic to the specialized smooth muscle cells. The second stage (anatomic closure) is usually completed in a few days to weeks after birth and results from (1) subendothelial deposition of extracellular matrix, (2) resorption of the internal elastic lamina and elastin fibers in the media, and (3) migration of undifferentiated smooth muscle cells into the subendothelial space. The ductus closes from the pulmonary end toward the aortic end, often leaving a “ductal ampulla” seen on echocardiography. The resulting nonpatent ductus is then called the ligamentum arteriosum. The patent ductus arteriosus (PDA) is defined as persistent patency of the fetal ductus arteriosus beyond its normal time of spontaneous closure.
RISK FACTORS FOR PATENT DUCTUS ARTERIOSUS
Any pathology that alters the molecular mechanisms of normal ductal closure may result in PDA. By far, the most frequently encountered risk factor for PDA is prematurity. The incidence of PDA increases with lower birth weight and estimated gestational age (EGA), reaching 77% at EGA 28 weeks. Circulating PGE2 activity is greater in the preterm infant than in the full-term infant, promoting persistent ductal patency, presumably because PGE2 is completely metabolized with first pass through the mature lung but incompletely in the premature lung. The risk for PDA is further increased with infant respiratory distress syndrome (RDS). Ninety percent of babies with RDS and <32 weeks EGA have PDA.
PATHOPHYSIOLOGY, CLINICAL MANIFESTATIONS, AND DIAGNOSIS
Premature Neonates
In premature neonates, the normal decrease in pulmonary vascular resistance with time leads to a left-to-right shunt, which results in pulmonary vascular overcirculation and an excess volume load on the left ventricle. If the shunt is large, clinically significant congestive heart failure can develop, leading to compromised pulmonary function and systemic cardiac output. Findings include pulmonary congestion, tachypnea, ventilator dependence, peripheral edema, and poor organ and tissue perfusion.
Lung immaturity confounds the relationship between PDA and these clinical manifestations. Pulmonary dysfunction may be due to RDS and bronchopulmonary dysfunction (BPD) and difficult to separate from the clinical effects of pulmonary overcirculation. Necrotizing enterocolitis may be related to microbial effects rather than to PDA. Discriminating the underlying causes has proven to be very difficult. Until an evidence-based guide to clinical impact is developed, McNamara and Sehgal have proposed a combined clinical and echocardiographic staging system for determining the “importance” of the hemodynamically significant PDA in the premature neonate, described in Table 77.1.
Full-Term Infants and Children
As in premature newborns, the principal pathophysiology of PDA is a left-to-right shunt leading to congestive heart failure. With large shunt, infants manifest failure to thrive, upper respiratory infections, and fatigue with exertion (including feeding). Physical examination shows a continuous “machinery murmur” in the left second intercostal space, bounding pulses, an overactive precordium, wide pulse pressure, and enlarged liver. Chest film shows increased vascular markings, interstitial edema, and enlarged cardiac silhouette. Echocardiography demonstrates the ductal and aortic arch anatomy, direction of flow, and evidence of chamber dilatation.
With a large shunt present for a sufficiently long time (but as little as 6 months), pulmonary vasculopathy may develop. Patients will have symptoms consistent with pulmonary hypertension (PAH). They may exhibit differential cyanosis due to flow reversal in the PDA. Echocardiography will confirm bidirectional or right-to-left flow in the PDA. With progressive vascular injury, PAH becomes irreversible, leading to Eisenmenger’s syndrome. Cardiac catheterization is indicated for any patient with PDA with clinical or echocardiographic suspicion of PAH.
Table 77.1 Representative “Staging System” for Determining the Magnitude of the Hemodynamically Significant Ductus Arteriosus Based on Clinical and Echocardiographic Criteria
Clinical
Echocardiography
C1 Asymptomatic
E1 No evidence of ductal flow on two-dimensional or Doppler interrogation
C2Mild
Hypoxemia (OI <6)
Occasional (<6) episodes of oxygen desaturation, bradycardia, or apnea Need for respiratory support (nCPAP) or mechanical ventilation (MAP <8) Feeding intolerance (>20% gastric aspirates)
Radiologic evidence of increased pulmonary vascularity
Moderate-to-severe metabolic acidosis (pH <7.1) or base deficit >−12.0
E4Large HSDA
Transductal diameter >3.0 mm
Unrestrictive pulsatile transductal flow
Severe left heart volume loading (e.g., LA:Ao ratio >2.1, mitral regurgitant jet >2.0 m/s)
Severe left heart pressure loading (e.g., E/A ratio >1.5 or IVRT >60)
Reversal of end-diastolic flow in superior mesenteric artery, middle cerebral artery, or renal artery
DA Vmax, ductus arteriosus peak velocity; E/A, early passive to late atrial contractile phase of transmittal filling ratio; HSDA, hemodynamically significant ductus arteriosus; IVRT, isovolumic relaxation time; LA:Ao ratio, left atrium to aortic ratio; MAP, mean airway pressure; nCPAP, nasal continuous positive airway pressure; NEC, necrotizing enterocolitis; OI, oxygenation index.
Modified from McNamara and Sehgal.
PDA with a small left-to-right shunt may be asymptomatic and produce no chamber enlargement. Even smaller PDAs may lack an audible murmur (so-called “silent ductus”) and are found incidentally on echocardiography or contrast studies.
In Adults
Adults with small, restrictive PDA may be asymptomatic and show no other pathological findings. Adults with anatomically large PDA may show signs of congestive heart failure or they may present with symptoms and signs of PAH or Eisenmenger’s syndrome, as described above. Rarely, an adult may present with infective endocarditis, ductal aneurysm, aortic or pulmonary aneurysm, or aortic dissection. Chest film and echocardiography may demonstrate calcification of the ductus.
NATURAL HISTORY
Premature Neonates
The natural history in this population is confounded by the coexisting morbidities of prematurity. No study clearly establishes PDA as a cause of death in this population. Spontaneous ductal closure continues to occur at least up to 1 year of age. In a study of 122 infants with birth weight <1,000 g, closure occurred within 3 days in 25, within 8 days in 42, and before hospital discharge in 46. Among infants with birth weight >1,000 g, the ductus closed without intervention in 67% by age 7 days and in 94% prior to discharge, at a median age of 7 days.
Children and Adults
The spontaneous closure rate in children >1-year old is about 0.6% per year. Among patients with significant sized PDA, the overall mortality in older patients with PDA at 0.49% per year (for age 2 to 19 years) and 1.8% per year (for age >20 years), 30% are dying from congestive heart failure. Patients with large, untreated PDAs that progress to severe PAH have survival curve typical for that of Eisenmenger’s syndrome. The risk of bacterial endocarditis is very low in the antibiotic era but not zero, even with a “silent ductus.”
TREATMENT
Historical Notes
The first successful PDA ligation was performed on a 7-year-old girl by Robert Edward Gross (1905 to 1988) on August 26, 1938. The history, along with some legend, is detailed by Alexi-Meskishvili and Böttcher. In 1966, Werner Porstmann (1921 to 1982) was the first to close a PDA by catheter technique. In 1976, Heymann, Rudolph, and Silverman first reported the use of indomethacin to close PDA in premature infants.
Indications for Treatment
Premature Neonates
The staging system proposed by McNamara and Sehgal (Table 77.1) is a reasonable guide to therapy—a “C3E4” patient would certainly be recommended for PDA closure in most neonatal centers. Most commonly, such a baby has (1) a large PDA with a large shunt, (2) refractory or worsening ventilator dependence and/or poor tissue perfusion in the absence of some other dominating and reversible cause, and (3) has failed a trial of COX inhibitors. Babies with stage C4 are a very high-risk group and the decision to undergo surgical ligation should be based on careful discussions with the neonatologists and parents. PDA management in babies with stage less severe than C3E3 is subject to the most debate.
The surgeon should understand the basis for uncertainty in the indications for PDA closure in this population. The primary reason is that, despite at least 75 randomized-controlled trials of interventions to close PDA in premature infants, there is scant evidence that either prophylactic or therapeutic PDA closure, either by medical or by surgical means, improves any clinical outcome measure. Taken individually, each of these randomized-controlled studies had weaknesses—most were small studies (<100 subjects), many had “rate of ductal closure” as their primary outcome measure and cross-over rates were frequently high. Only 17 of the 75 trials were conducted after the advent, in 1989, of exogenous surfactant therapy. Benitz, in 2010, attempted a meta-analytic study of these trials. Such an approach mathematically narrows the confidence intervals of odds ratios for the chosen outcomes, but it widens the underlying variability of the covariates. The Cochrane Reviews apply more stringent criteria to selection of studies for meta-analysis, eliminating studies with significant methodological deficiencies. The reviewers found only one eligible study pertaining to prophylactic surgical ligation of PDA, which showed that ligation decreased the incidence of NEC but had no long-term effect on mortality or BPD incidence. Furthermore, the reviewers found only one eligible study pertaining to surgical ligation for the treatment of PDA, concluding that this study contained insufficient data to evaluate the effectiveness of the intervention. Thus, as of year 2011, there are no studies, properly designed and containing sufficient data that evaluate surgical ligation for the treatment of PDA in premature infants.
Full-term infants: In full-term infants >6 to 12 months old, occlusion of an audible PDA with left-to-right flow is reasonable. PDA occlusion is also indicated at any age when the PDA is moderate to large and produces congestive heart failure. Infants and children with PDA undergoing other cardiac or thoracic operations should undergo simultaneous PDA ligation.
Children and Adults
Beyond infancy, probably the spontaneous ductal closure is low. Audible PDA with left-to-right flow should be occluded. Recommendations for PDA closure in adults are further described in the American College of Cardiology/American Heart Association 2008 Guidelines for Adults with Congenital Heart Disease (ACC/AHA).
Contraindications to Treatment
PDA should not be occluded in patients with PAH associated with significant pulmonary vascular obstructive disease (PVOD). At cardiac catheterization, if pulmonary vascular resistance index is greater than eight Woods units per meter squared and does not decrease with oxygen, nitric oxide, or other pulmonary vasodilators, then PDA closure is contraindicated. Indications for PDA closure in the presence of some reactivity of PAH are controversial.
In premature neonates, bidirectional flow in a PDA is not a contraindication to ligation. PDA should not be ligated as an isolated procedure in the presence of “ductal dependent circulation.” The treatment of an inaudible PDA is not contraindicated but is controversial.
Medical Treatment
COX inhibitors close PDA in premature neonates in about 70% of cases, a significantly lower success rate than the closure rate of surgical ligation. Complications are reported for all COX inhibitors, including ibuprofen, in this population. COX inhibitors are not effective in closing PDA beyond a few weeks of age.
Catheter-Based Treatment
Catheter-based occlusion of PDA is an acceptable method of treatment in some cases. The choice of device is often made on the basis of the classification of Krichenko et al. Gianturco or Flipper coils are generally deployed by the femoral artery approach and used for types D and E, or ductus <2 mm diameter. The Amplatzer vascular plug IV is deployed usually via the femoral vein and is applicable for types C, D, and E. Finally, the Amplatzer II occluder device (ADO) is usually deployed via the femoral vein and applicable for type A. In patients <10 kg, this device may obstruct the aorta. In large diameter or short PDA, the incidence of residual flow has been shown to be less with the ADO than with coils.
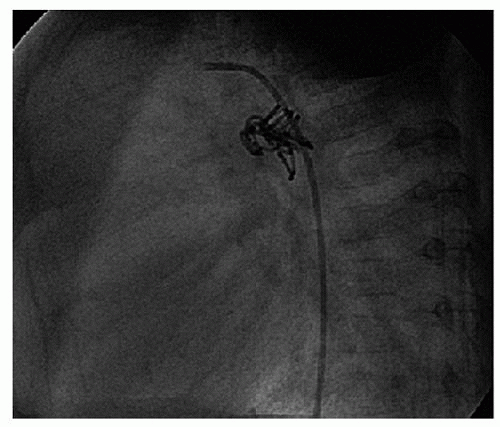
Complications of catheter-based PDA occlusion include femoral artery pseudoaneurysm, limb ischemia, device embolization, left pulmonary artery stenosis, endarteritis, radiation exposure risks, dye-induced renal dysfunction, residual ductal flow, device-related hemolysis, descending aortic obstruction, hemorrhage, need for transfusion, and failure to complete the procedure (Fig. 77.1). The precise incidences of these complications are not well known due to the paucity of published data from catheterization registries, multi-institutional studies, or Cochrane reviews. The incidence of device embolization is approximately 2% and that of residual flow is 1.4% to 7%. Hemolysis typically occurs with incomplete ductal closure, though it can also occur with complete occlusion. The incidence of complications during and after catheter interventions of all types has been estimated to be nearly 20%.
Experience with catheter-based PDA occlusion has extended to smaller infants and even premature neonates. Long-term outcomes were not determined in these series.
Fig. 77.1. Gianturco coils occluding the descending aorta after attempted coil occlusion of patent ductus arteriosus. The Doppler gradient was 40 mmHg. Through a lateral thoracotomy, proximal and distal aortic control was achieved, a short aortotomy made, and the coils removed. The PDA was doubly ligated.
Catheter-based closure of PDA is effective in adults and preferred in adults with calcified PDA or with significant other medical problems. Relative contraindications include the presence of ductal aneurysm or active ductal/pulmonary arterial endarteritis. Case reports of the use of covered aortic stents have recently appeared. This approach may be appropriate for the large or aneurismal ductus.
In infants and children, catheter-based PDA occlusion has been compared with open surgical ligation. Total complication rates are similar, but coil occlusion is less costly than open
Only gold members can continue reading. Log In or Register to continue
 TREATMENT
TREATMENT