Chapter 9 Myocardial Infarction and Ischemia, II Non–ST Segment Elevation and Non–Q Wave Syndromes
Please go to expertconsult.com for supplemental chapter material.
Myocardial infarction (MI) may be associated with abnormal Q waves associated with the typical progression of ST segment elevation myocardial infarction (STEMI) and T wave inversions described in Chapter 8. In many cases, however, myocardial ischemia (with or without actual infarction) may be limited primarily to the subendocardium (inner layer) of the ventricle, often associated with ST segment depressions, rather than primary ST elevations.
Subendocardial Ischemia
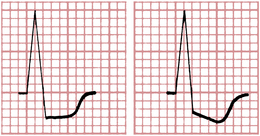
The most common ECG change with subendocardial ischemia is ST segment depression (Fig. 9-1). The ST depression may be limited to the anterior leads (I, aVL, and V1 to V6) or to the inferior leads (II, III, and aVF), or it may be seen more diffusely in both groups of leads. As shown in Figure 9-1, the ST segment depression with subendocardial ischemia has a characteristic squared-off shape. (ST segment elevation is usually seen in lead aVR.)
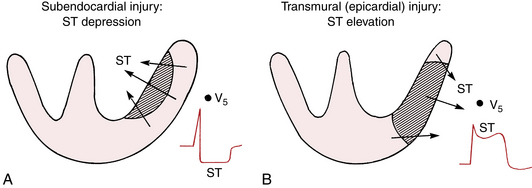
Recall from Chapter 8 that acute transmural ischemia produces ST segment elevation, a current of injury pattern. This results from epicardial injury. With pure subendocardial ischemia, just the opposite occurs; that is, the ECG shows ST segment depression (except in lead aVR, which often shows ST elevation).
In summary, myocardial ischemia involving primarily the subendocardium usually produces ST segment depression, whereas acute ischemia involving the epicardium usually produces ST elevation. This difference in the direction of the injury current vector is depicted in Figure 9-2.
ECG Changes with Angina Pectoris
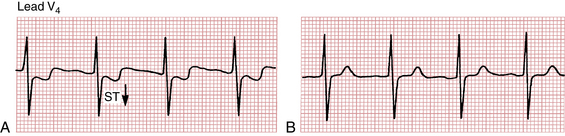
Many (but not all) patients with classic angina have an ECG pattern of subendocardial ischemia, with ST segment depressions seen during an attack. When the pain disappears, the ST segments generally return to the baseline. (Fig. 9-3 shows ST depressions during a spontaneous episode of angina.)
Exercise (Stress) Testing and Coronary Artery Disease
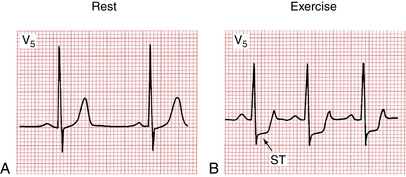
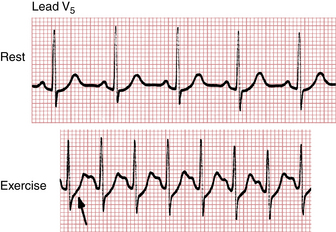
Figure 9-4A is the normal resting ECG of a patient, whereas Figure 9-4B shows the marked ST depressions recorded while the patient was exercising. The appearance of ST segment depressions constitutes a positive (abnormal) result. Most cardiologists accept horizontal or downward ST depressions of at least 1 mm or more, lasting at least 0.08 sec (two small boxes) as a positive (abnormal) test result (see Fig. 9-4B). ST depressions of less than 1 mm (or depressions of only the J point) with a rapid upward sloping of the ST segment are considered a negative (normal) test response (Fig. 9-5).
The finding of prominent ischemic ST changes, with or without symptoms, occurring at a low level of activity is particularly ominous. Sometimes, these changes will be associated with a drop in blood pressure. These findings may indicate severe three-vessel coronary disease and sometimes high-grade obstruction of the left main coronary artery.
False-positive tests (defined here as ST depressions without obstructive coronary disease) can also be seen in patients who are taking digitalis and in patients who have hypokalemia, left ventricular hypertrophy (LVH), ventricular conduction disturbances, or a Wolff-Parkinson-White pattern (see Chapter 12).
“Silent” Myocardial Ischemia
A patient with coronary artery disease may have episodes of myocardial ischemia without angina, hence the term silent ischemia. Silent ischemia is sometimes detected during exercise testing. Ambulatory ECG (Holter) monitoring is the most useful way of assessing silent myocardial ischemia (see Chapter 3). The 24-hour ECG monitoring of patients with coronary artery disease reveals a surprisingly high frequency of ST depressions not associated with angina. This important topic is discussed again later in this chapter.



