Table 12.1 Etiology of Mitral Valve Disease | ||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||
leaflets. The posteromedial papillary muscle provides chordae to the posteromedial aspect of both leaflets. There is substantial variability in the exact number of chordae and the percentage of chords that are devoted to the anterior and posterior leaflets, but in general both papillary muscles provide chordal attachments to a portion of each of the leaflets. The posteromedial papillary muscle typically is perfused by the right coronary artery, and the anterolateral papillary muscle has a dual blood supply. Because of the dual blood supply of the anterolateral papillary muscle, it is less susceptible to ischemic injury than the posteromedial papillary muscle.
Table 12.2 Appropriateness Criteria for Use of Echocardiography in Mitral Valve Disease | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
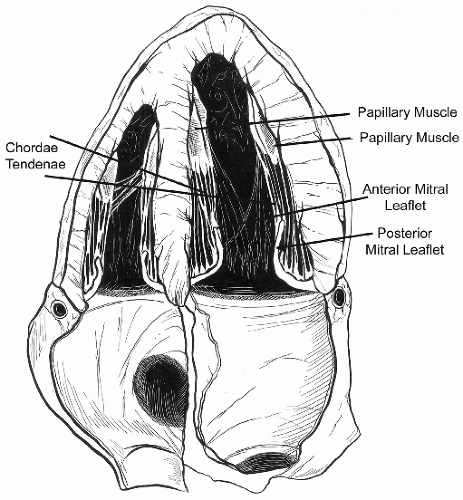 FIGURE 12.1. Anatomic rendering of the normal mitral valve apparatus. Note that the chordae are attached not only to the tips of the mitral valve leaflets but also to the mid portion of the leaflets. (Artwork by Amanda Almon and Travis Vermilye.) |
Table 12.3 Anatomic Correlates of Disease of the Mitral Valve | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
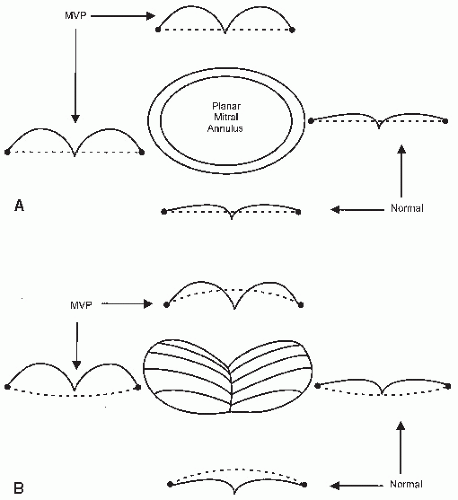 FIGURE 12.2. Schematic representation of a hypothetical planar mitral valve annulus (A) and the more accurate three-dimensional geometry of the annulus (B). In each set of schematics, the plane of the annulus is depicted as a dotted line and either a normal mitral valve or a mitral valve with mitral valve prolapse, depicted as viewed from orthogonal planes. A: Note that a planar annulus results in the same appearance of the mitral valve when viewed from two perspectives 90° apart. Normal mitral closure is noted on the right and the bottom of each schematic and mitral valve prolapse at the top and left. Note that the normal valve closes with the belly of the leaflet slightly behind the plane of the annulus, irrespective of the viewing perspective, and that the prolapse valve bows to a substantially greater degree. B: Because of its complex three-dimensional shape, the annulus may be either concave or convex toward the apex of the left ventricle depending on the viewing perspective. With a normal closure pattern in the lower annular schematic, note that the leaflet does not protrude above the plane of the annulus. The schematic to the right represents the identical closing geometry of the mitral valve, which now appears to prolapse behind the plane of the annulus because of its geometry in that perspective. The upper and leftward schematics depict the appearance of mitral valve prolapse as it relates to the saddle-shape geometry. In each instance, the geometry of the prolapse schematic is identical. Note the substantially greater degree to which prolapse is apparent on the left in B versus in A, which is related to the different contour of the annulus when viewed from the orthogonal views. MVP, mitral valve prolapse. |
 FIGURE 12.3. Schematic representation of the mitral valve from multiple perspectives. Bottom: The view of the mitral valve in a surgical approach from inside the left atrium. Top: The mitral valve as viewed from a traditional transthoracic parasternal short-axis view. Middle: The mitral valve is seen from a transesophageal approach at the mid gastric level. In each instance, the proximal aorta is as noted in the schematic, as is the left atrial appendage. The three distinct scallops of the anterior and posterior leaflets (A1, A2, A3, P1, P2, P3) are also schematized. L, left coronary sinus; N, noncoronary sinus; R, right coronary sinus. |
12.14 and 12.15 show substantial fibrosis or calcification. In Figure 12.16, diffuse thickening and fibrosis of the entire extent of the leaflets and chordae are shown.
 FIGURE 12.4. Expanded view of the mitral valve as seen from a transthoracic echocardiographic approach. This image corresponds to the top image of Figure 12.3. The imaging plane of a traditional transverse (0°) plane and parasternal long-axis view (or 120° transesophageal echocardiographic view) are as noted. Note that when imaged from a 60° imaging plane (commissural view) with a transesophageal echocardiographic probe, the imaging plane will intersect the P1, A2, P3 intersection. A1, A2, A3, anterior scallops 1 through 3; L, left coronary sinus; N, noncoronary sinus; P1, P2, P3, posterior scallops 1 through 3; PLAX, transthoracic parasternal long-axis plane; R, right coronary sinus; TEE, transesophageal echocardiography. |
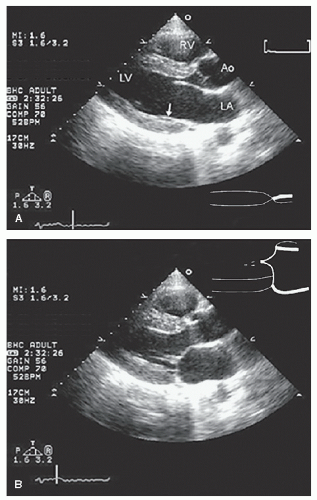 FIGURE 12.5. Parasternal long-axis view recorded in diastole (A) and systole (B) in a patient with a normal mitral valve. A: Note the anterior and posterior mitral valve leaflets. The posterior leaflet lies against the inferoposterior wall of the left ventricle (arrow) and may not be clearly seen when fully open. B: Both leaflets have moved toward the center of the left ventricular cavity and have closed with a 2- to 3-mm zone of overlap (the zona coapta). This is schematized in the middle to the right. |
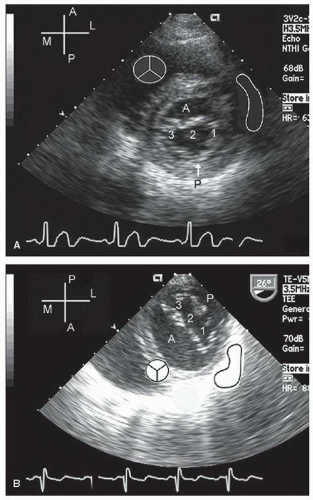 FIGURE 12.6. Parasternal short-axis view (A) and transesophageal short-axis view from a transgastric position (B) recorded in normal patients. The positions of the aorta and left atrial appendage are as noted by the schematics. In each of these examples, recorded in diastole, the anterior (A) and posterior (P) leaflets of the mitral valve are clearly visualized and the three distinct regions (1-3) can be seen. For each imaging format, notice that the A1/P1 coaptation point is closest to the left atrial appendage and the A3/P3 coaptation closest to the ventricular septum. M, medial; L, lateral. |
 FIGURE 12.7. Apical four-chamber view recorded in systole in a normal patient. In this image, the normal closure pattern of the anterior and posterior leaflets of the mitral valve is clearly demonstrated. At the upper right, the closure pattern has been expanded. Note that the anterior and posterior mitral valve leaflets do not close tip to tip but rather along a 4-mm length (the zona coapta [ZC]). |
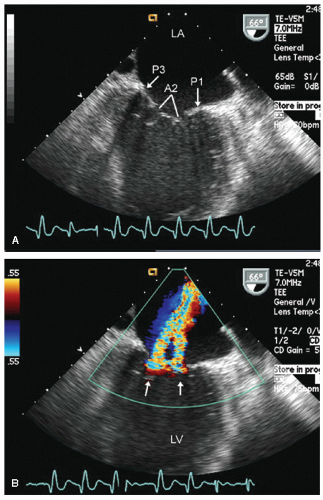 FIGURE 12.8. Transesophageal echocardiogram recorded at 66°. In this view, the P1, A2, and P3 scallops are clearly visualized (A). B: Note the two separate mitral regurgitation jets (arrows) arising from the P1-A2 and P3-A2 commissures. A1, A2, A3, anterior scallops 1 through 3; P1, P2, P3, posterior scallops 1 through 3. |
 FIGURE 12.9. Anatomic rendering of the normal mitral valve in a closed position. Again note the chordae that attach not only to the leaflet tips but to the belly of the leaflet as well. Also note that the normal mitral valve does not close in a tip-to-tip manner but that there is an overlap of the leaflets as they close (the zona coapta). (Artwork by Amanda Almon and Travis Vermilye.) |
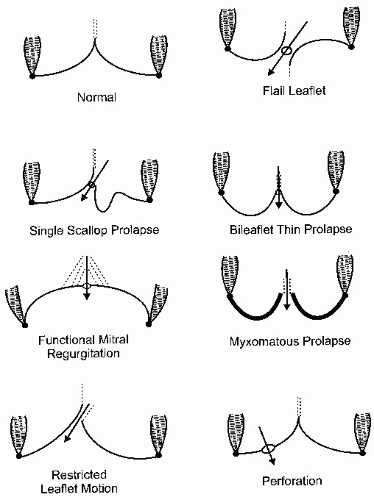 FIGURE 12.10. Schematic drawings demonstrate a normal mitral valve closure pattern (upper left) and multiple different pathologic closure patterns. In each example, the annulus (small black dot) and proximal ventricular wall are denoted. At the point of the intended coaptation, the open circle denotes the regurgitant orifice and the arrow denotes the direction of the regurgitant flow. The dotted lines denote the mitral valve chordae. |
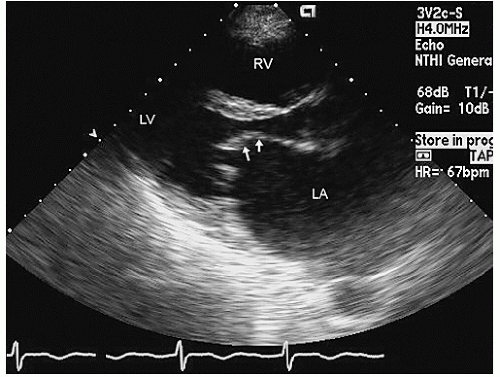 FIGURE 12.11. Transthoracic parasternal long-axis view echocardiogram recorded in a patient with rheumatic mitral stenosis. In this image, recorded in early diastole, note the doming motion of the anterior mitral valve leaflet with restriction of motion at the tips. The belly of the leaflet (arrows) is pliable, and there is little or no fibrosis, calcification, or thickening of the leaflets. Also note the secondary dilation of the left atrium. In the real-time image, note the relatively fixed position of the leaflet tips with all motion of the leaflet occurring at the mid and proximal portions of the leaflets. |
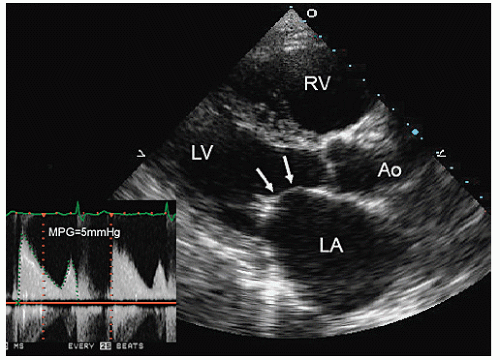 FIGURE 12.12. Parasternal transthoracic echocardiogram recorded in a patient with rheumatic mitral valve stenosis. The image frame was recorded in diastole and shows classic “doming” of the anterior mitral leaflet (arrows) as well as the dilated left atrium. Note the somewhat greater degree of focal thickening at the tips of the leaflets in comparison to Figure 12.11. Continuous wave Doppler showed a transmitral gradient of 5 mm Hg across the valve from an apical position (inset) MPG, mean pressure gradient. |
 FIGURE 12.13. Parasternal long-axis view (A) and apical four-chamber view (B) recorded in a patient with mitral stenosis. A: Note the marked doming of the mitral valve in diastole with focal thickening at the tips of both the anterior and posterior leaflets. In the real-time image, note that pliability of the mid portion of the mitral valve. B: Apical four-chamber view reveals a similar phenomenon with doming of the mitral valve in diastole toward the apex. |
of rheumatic heart disease on M-mode echocardiography was increased echogenicity of the leaflets with decreased excursion and reduced separation of the anterior and posterior leaflets. This was accompanied by a reduced diastolic (E-F) slope of mitral closure (Fig. 12.18). The E-F slope could be measured in millimeter per second and followed after intervention (the only intervention available at the time that this measurement was commonly undertaken was open mitral commissurotomy). The E-F slope was inversely correlated with the severity of mitral stenosis and improved (i.e., became steeper) after successful commissurotomy. The E-F slope ultimately proved to be nonspecific and was noted in situations in which left ventricular filling was impaired such as in diastolic dysfunction. The E-F slope is of more historical than clinical value today. Additional features of mitral stenosis noted on M-mode echocardiography included “paradoxical” anterior diastolic motion of the posterior mitral valve leaflet. This occurred because tethering at the tips resulted in an obligatory anterior motion of the posterior leaflet tips that tethered to the larger anterior leaflet. M-mode echocardiography has been replaced by two-dimensional echocardiography and Doppler techniques as a means of diagnosing and quantifying mitral stenosis.
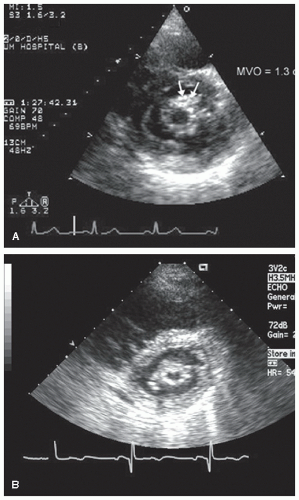 FIGURE 12.14. Parasternal short-axis views recorded in patients with rheumatic mitral stenosis. In each instance, note the restricted mitral valve orifice. A: The orifice can be planimetered as 1.3 cm2. In this example, note the localized thickening of the chordae at the anterolateral border of the mitral orifice (arrows). B: Recorded in a patient with more severe stenosis. The mitral orifice has been planimetered at 0.7 cm2. Also note the diffuse nature of thickening around the mitral orifice. MVO, mitral valve orifice. |
 FIGURE 12.15. Apical four-chamber view recorded in a patient with rheumatic mitral stenosis. Note the marked dilation of the left atrium. In this example, there is substantial, focal calcification of the anterior mitral valve leaflet (arrow). Note also the relatively restricted motion of both leaflets along their full length. |
 FIGURE 12.16. Parasternal long-axis (A) and short-axis (B) transthoracic echocardiograms recorded in a patient with rheumatic mitral stenosis. A: Note the marked thickening of the chordae throughout their entire length, from the mitral leaflet to the papillary muscles. In the short-axis view (B), the slit-like orifice of the mitral valve is visualized. |
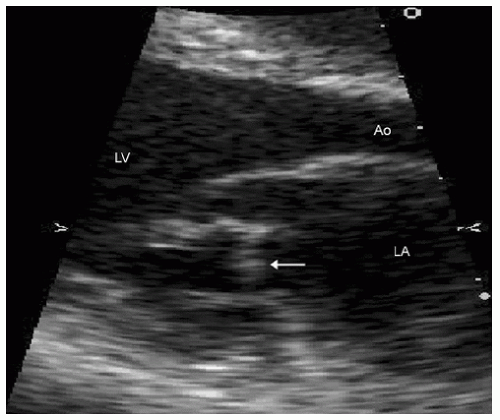 FIGURE 12.17. Expanded parasternal long-axis view recorded in a young patient with congenital mitral stenosis. Note the abnormal position of chordae to the posterior mitral leaflet (arrow), which restricts its motion, resulting in mitral stenosis. IVS, interventricular septum. |
involvement when the mitral valve is viewed from the left atrial aspect. Use of transgastric planes in 90° to 120° views can provide detailed visualization of the chordal apparatus (Figs. 12.19, 12.20 and 12.21).
 FIGURE 12.18. M-mode echocardiogram recorded in a patient with rheumatic mitral stenosis. Note the marked thickening of the mitral valve leaflets and the flat E-F slope during diastole. The posterior leaflet appears to move anteriorly in diastole as well. |
 FIGURE 12.19. Transesophageal echocardiogram recorded in transverse and longitudinal views in a patient with mitral stenosis. A, B: In both images, note the diffuse thickening of the mitral leaflets with the doming motion in diastole. B: Also note the diffuse thickening of the chordae (arrows). |
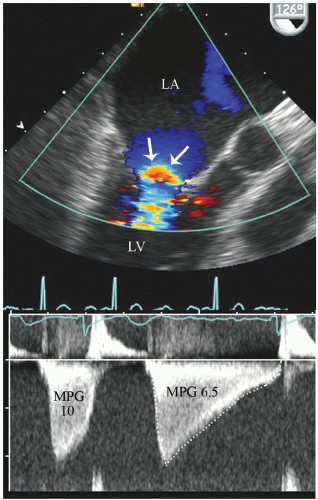 FIGURE 12.20. Transesophageal echocardiogram recorded from a 126° imaging angle from behind the left atrium. Note the doming of the mitral valve in diastole and the color flow convergence zone within the left atrium (arrows) as flow accelerates toward the restricted orifice. The continuous wave Doppler through the restricted orifice is also presented revealing mean transvalvular gradients of 10 and 6.5 mm Hg for the shorter and longer cycles in this patient with atrial fibrillation. MPG, mean pressure gradient. |
from this approach. First, one should recognize that, in mitral stenosis, the mitral valve represents a funnel-shaped structure that tapers to its limiting orifice at the tips and careful scanning must be performed to ensure that the image is frozen and planimetered at the mitral valve tips and not more proximally where the orifice area would be overstated (Fig. 12.24). Second, instrumentation gain, reject, and transmission power all affect the ability to accurately visualize the limiting orifice. Increased gain will result in a “blooming” of the echoes, which then overstates their boundary and thereby diminishes the visualized orifice. When appropriately recorded, the measured orifice area correlates very well with that determined by hemodynamics. After commissurotomy, the orifice often becomes more irregular and the area of the commissural opening may be difficult to planimeter accurately.
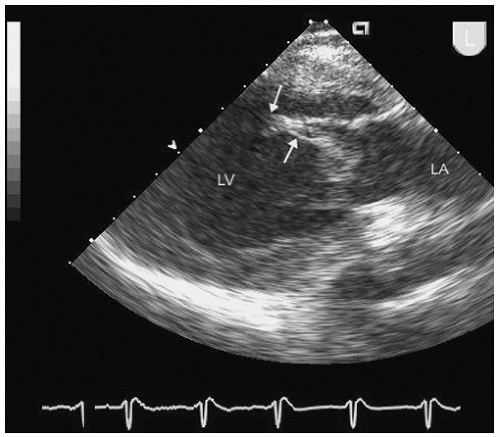 FIGURE 12.21. Transesophageal echocardiogram recorded in a longitudinal view in a patient with rheumatic mitral stenosis. Note the diffuse thickening of the chordae and fibrosis of the papillary muscle tip (arrows). |
 FIGURE 12.22. Real-time transesophageal three-dimensional echocardiogram recorded from a left atrial perspective in a patient with rheumatic mitral stenosis. Notice the diffuse thickening of the leaflets and the crescent-shaped mitral valve orifice (MVO) noted in both the illustrated schematic and real-time image. |
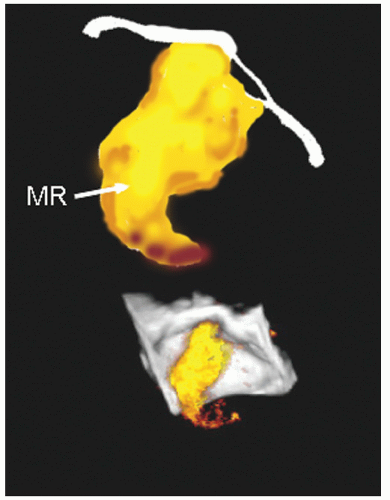 FIGURE 12.23. Three-dimensional echocardiogram with color flow Doppler recorded in a patient with rheumatic mitral stenosis. In the lower panel, note the diffuse thickening and doming of the mitral leaflets and the jet of mitral regurgitation, also schematized in the upper panel. The restricted doming motion of the mitral leaflets are best appreciated in the accompanying real-time image. MR, mitral regurgitation. |
provides suboptimal anatomic definition of the mitral valve. The transmitral gradient should be recorded using continuous wave Doppler imaging aligned as parallel as possible to the anticipated flow. If pulsed wave Doppler imaging is used, it is essential that the sample volume be placed at the level of the restrictive orifice and not further back near the annulus. Placement of the sample volume near the annulus will result in systematic underestimation of the transmitral gradient. In general, rheumatic mitral stenosis results in a central stenotic orifice with flow directed from the left atrium toward the apex of the left ventricle. As such, traditional two- and four-chamber viewing planes usually suffice for measurement. If necessary, color flow imaging can be used to determine the direction of flow and further refine this assessment. The peak and mean pressure gradient can be obtained online by electronic planimetry of the spectral profile (Fig. 12.26). Atrial fibrillation with an irregular heart rate poses additional problems. Depending on the diastolic filling time, there may be dramatic variation in the mean transvalvular gradient and multiple cycles should be averaged to provide an accurate assessment of severity (Fig. 12.27).
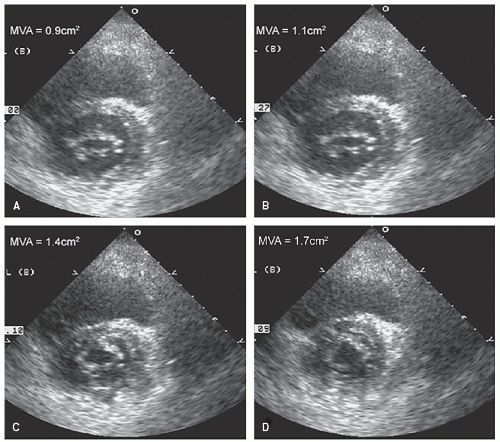 FIGURE 12.24. Series of parasternal short-axis views recorded in a patient with rheumatic mitral stenosis. A: Recorded at the actual restrictive orifice, and the mitral valve area (MVA) can be planimetered at 0.9 cm2. B-D: The three additional views were recorded progressively closer to the annulus and show a progressive increase in the planimetered mitral orifice depending on the position at which the “orifice” is planimetered. |
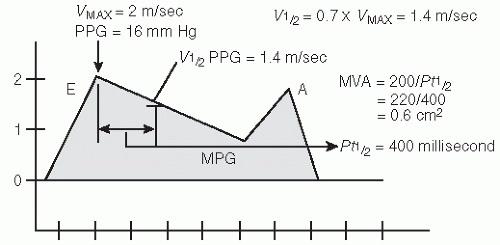 FIGURE 12.25. Schematic representation of mitral valve inflow depicting different parameters that can be extracted for determination of the severity of mitral stenosis. In the schematic, note the relatively flat decay of pressure from the E point. Parameters that can be measured include integration of the overall pressure gradient beneath the spectral display to calculate the mean pressure gradient (MPG) as well as calculation of mitral valve area (MVA) from the pressure half-time method. For the pressure half-time method, the time required for the pressure to decay from its peak value (16 mm Hg in this example) to one half of that value (8 mm Hg) is determined. The velocity at which the gradient has declined to one half its peak can be calculated as 0.7 × VMAX. This value (400 milliseconds in this example) is then entered into the equation MVA = 220/Pt½. In the schematic, the MVA calculates to 0.6 cm2. PPG, peak pressure gradient. |
either left atrial driving pressure or left ventricular compliance and pressure. Situations in which the latter can be altered include left ventricular hypertrophy or concurrent aortic insufficiency, in which there is competitive filling of the left ventricle. In many instances, the mitral stenosis signal does not have a uniform slope but may have an early rapid decay followed by a more gradual decay, giving a “ski slope” appearance. In this instance, caution is advised, but the more accurate reflector of area will be derived from the flatter portion of the spectral envelope. In general, the derived anatomic area from the pressure half-time calculation is often less valuable for patient management than determination of pressure gradients and anatomically measured valve areas.
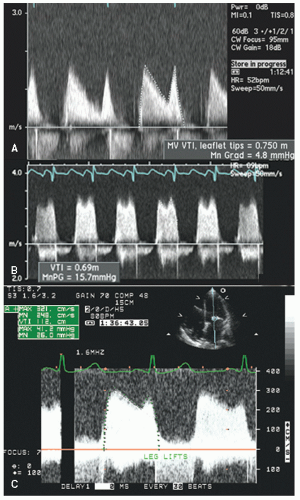 FIGURE 12.26. Transmitral Doppler tracings recorded in patients with varying degrees of mitral stenosis. A: Recorded in a patient with mild mitral stenosis. Note the relatively brisk pressure gradient decay and a mean gradient of 4.8 mm Hg. B: Recorded in a patient with more severe mitral stenosis and a mean gradient of 15.7 mm Hg. C: Recorded in a patient with severe mitral stenosis and a mean pressure gradient of 26 mm Hg after leg lifts. Also note the flat slope of pressure decay in this instance. |
(Fig. 12.29). On occasion, this exaggerated early pressure gradient, compared with the mean pressure gradient, can be a clue to the presence of concurrent mitral regurgitation in situations in which the mitral regurgitation may not be directly visualized. This observation may be of particular value in patients with highly eccentric regurgitation jets or paravalvular regurgitation in a mitral prosthesis.
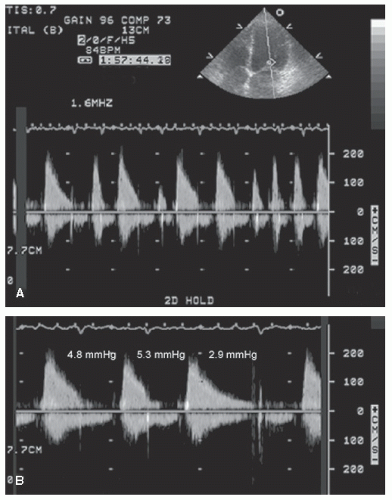 FIGURE 12.27. Transmitral continuous wave Doppler image recorded in a patient with mitral stenosis in atrial fibrillation with an irregular ventricular response. A: Note the marked variation in diastolic filling time and the obvious variation in the spectral profile. B: Recorded in the same patient, revealing three different diastolic filling profiles. Note the marked variation in the mean pressure gradient, dependent on diastolic filling time. MVA, mitral valve area. |
 FIGURE 12.28. Transmitral spectral Doppler image recorded in patients with mitral stenosis. Images recorded in a patient with relatively mild stenosis (A) and in a patient with more severe mitral stenosis (B). In each example, the pressure half-time has been used to calculate the mitral valve area, which is as noted on the figure. At the top, note the relatively steep decay of the pressure curve compared with the relatively flat pressure decay at the bottom. |
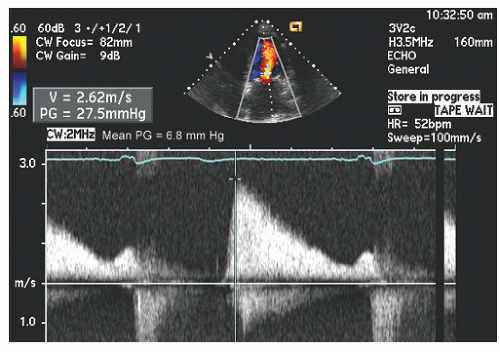 FIGURE 12.29. Transmitral Doppler image recorded in a patient with concurrent mitral stenosis and mitral regurgitation. Note the high peak early gradient (27.5 mm Hg) but the rapid decay and a negligible pressure gradient at end-diastole. Compare the peak early gradient of 27.5 mm Hg with the mean gradient of only 6.8 mm Hg. This discrepancy between peak and mean pressure gradient is often seen in patients with concurrent mitral regurgitation. |
recorded in patients with rheumatic mitral stenosis and varying degrees of spontaneous echo contrast and thrombus formation within the left atrium and left atrial appendage. Current opinion suggests that dense spontaneous echo contrast and stasis of blood are precursors to thrombus formation and are markers of a patient with increased thromboembolic risk, especially if seen in the presence of atrial fibrillation. Using pulsed Doppler, it is common to see reduced atrial appendage velocities in this setting (Fig. 12.36).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


