Table 23.1 Normal Variants and Benign Conditions Often Misinterpreted as Pathologic | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
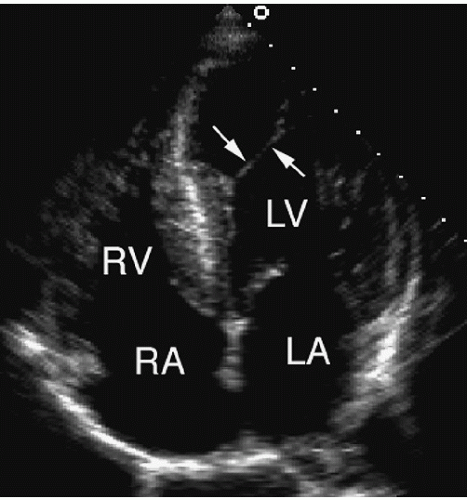 FIGURE 23.1. An apical four-chamber view demonstrates a false tendon (arrows) in the left ventricular apex. |
 FIGURE 23.2. A moderator band (arrow) is seen in the apex of the right ventricle. |
Table 23.2 Echocardiography in Patients with Cardiac Masses and Tumors | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
Table 23.3 Relative Frequency of Primary Cardiac Tumors | ||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||
with thrombi, although their characteristic location and attachment site is generally helpful in the differential diagnosis. After surgical excision, myxomas can recur. Therefore, surveillance echocardiograms should be obtained annually for several years to guard against this possibility.
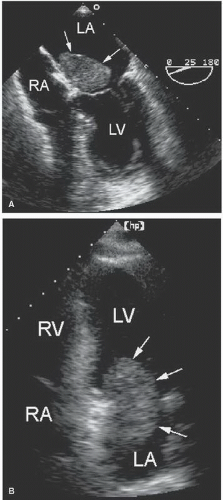 FIGURE 23.3. A: A myxoma (arrows) is seen in the left atrium on transesophageal imaging. The mass is attached to the fossa ovalis. B: A four-chamber view demonstrates a large myxoma within the left atrium partially obstructs the mitral orifice during diastole. |
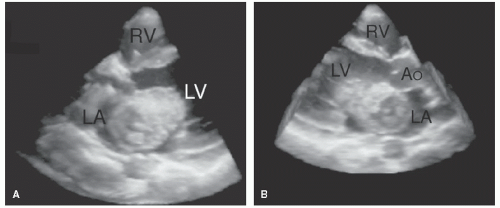 FIGURE 23.4. A large left atrial myxoma is demonstrated using three-dimensional imaging. The advantages of this modality are best appreciated when viewed in a cine loop format. |
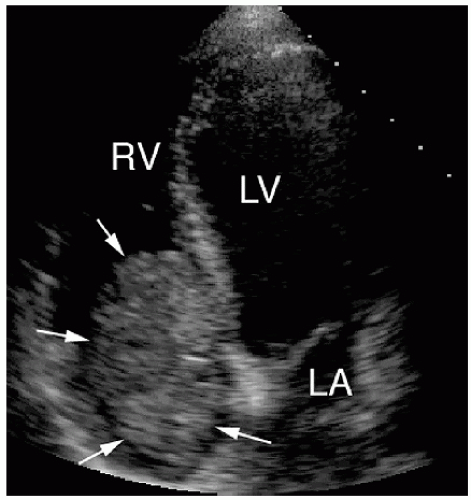 FIGURE 23.5. A large right atrial myxoma (arrows) is indicated by the arrows. The mass extends through the tricuspid valve into the right ventricle. |
 FIGURE 23.6. Upper left: A large mass is seen within the right atrium. Upper right: In diastole, note how the mobile mass protrudes through the tricuspid valve creating obstruction to right ventricular inflow. Lower panel: The degree of obstruction is demonstrated with pulsed Doppler, mean gradient = 9 mm Hg. The location, motion, and attachment site are consistent with right atrial myxoma. |
common and generally considered a risk factor for embolization. Significant valvular regurgitation is rare. There is some confusion as to whether fibroelastomas are distinct from Lambl’s excrescences, which are smaller and frequently seen on otherwise normal valves in elderly patients (Fig. 23.10). Whether the two represent the distinct entities remains controversial. Fibroelastomas are also confused with blood cysts, which are unusual blood-containing cystic structures that develop within mitral leaflets (Fig. 23.11). Blood cysts have a broader base, are sessile, and are less mobile than fibroelastomas. Papillary fibroelastomas may be detected as an incidental finding on echocardiography. Because tumors can act as a nidus for the formation of fibrin-platelet aggregates, embolic events have been attributed to papillary fibroelastomas.
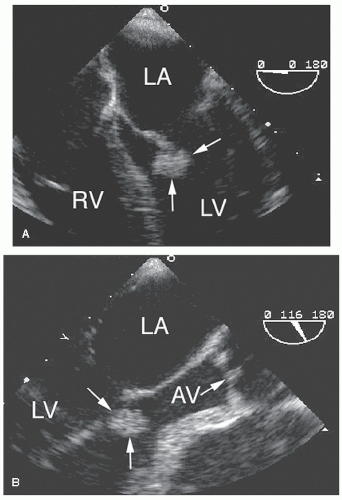 FIGURE 23.7. A transesophageal echocardiogram of the four-chamber (A) and long-axis (B) view show a papillary fibroelastoma of the mitral valve. The tumor was attached by a small pedicle to the anterior leaflet and was highly mobile. AV, aortic valve. |
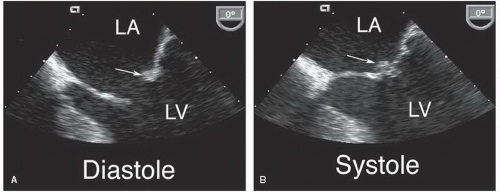 FIGURE 23.8. A small papillary fibroelastoma is seen in a patient who had a stroke. The mass (arrow) is seen on the posterior leaflet in diastole (A) and systole (B). |
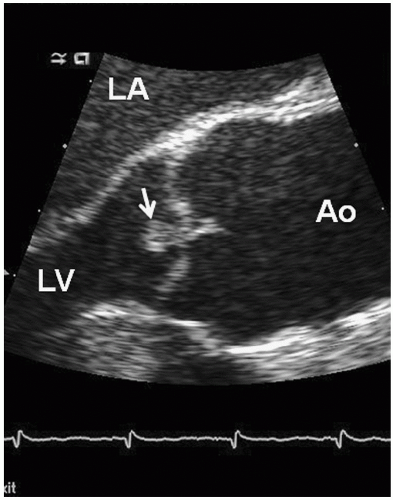 FIGURE 23.9. A transesophageal long-axis view of the aortic valve is shown from a patient who presented for evaluation of chest discomfort. The small, mobile mass attached to the aortic valve is a papillary fibroelastoma (arrow). |
of the fossa ovalis (Fig. 23.12). The fatty infiltrate is highly echogenic and results in a “dumbbell-shaped” appearance on two-dimensional echocardiography. The condition is thought to be benign and rarely associated with clinical manifestations.
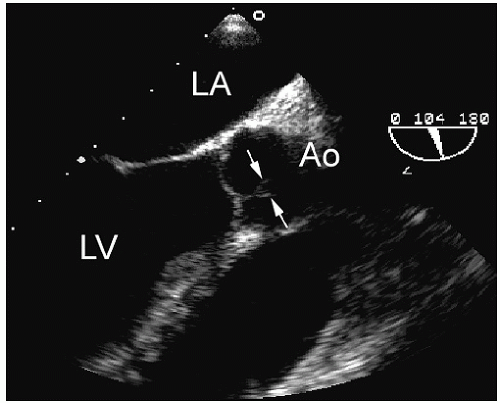 FIGURE 23.10. An example of Lambl’s excrescence of the aortic valve (arrows). |
Figure 23.15 is an example of a fibrosarcoma that occupies the right ventricular outflow tract. Its size and location combine to produce a significant outflow tract gradient, as evidenced by the Doppler recording. Such tumors tend to invade or replace myocardial tissue and thereby dramatically alter the appearance and/or function of the heart. A sarcoma involving the right and left atria is shown in Figure 23.16. The extension of the tumor through the atrial septum is suggestive of its malignant nature. As opposed to the well-circumscribed appearance of benign tumors, cardiac malignancies appear to infiltrate the tissues, disrupting normal anatomic planes, and invade or obliterate contiguous structures. The heart often appears tethered and relatively immobile, without its normal translational motion (Fig. 23.17). Contrast perfusion imaging may have a role in further characterizing intracardiac masses and distinguishing tumors from thrombi. Enhancement of the mass after contrast injection correlates with the degree of vascularity. Thus, malignant tumors and other vascular structures often demonstrate hyperenhancement while thrombi and other avascular masses, such as myxomas, show less contrast uptake.
 FIGURE 23.11. A blood cyst (arrow) within the anterior mitral leaflet. The cyst is relatively immobile and the attachment is broad based. The mass is seen during diastole (A) and systole (B). |
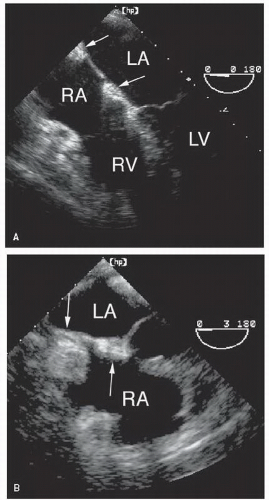 FIGURE 23.12. Lipomatous hypertrophy of the atrial septum. A: A mild degree of accumulation of lipomatous material is present (arrows). The fossa ovalis is characteristically spared. B: A more extreme form of lipomatous hypertrophy (arrows). |
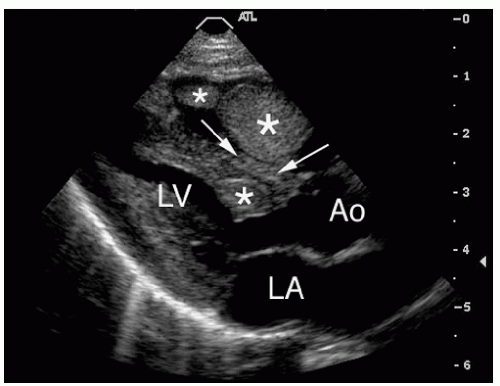 FIGURE 23.13. Rhabdomyoma is a common pediatric tumor. In this 12-year-old patient, multiple tumors are seen within the left and right ventricle (asterisks) and interventricular septum (arrows). |
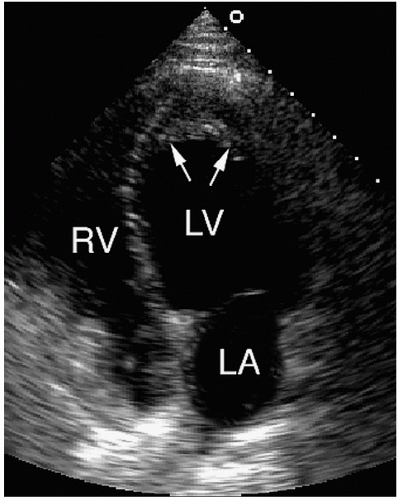 FIGURE 23.14. An example of endocardial fibroelastosis. Endocardial thickening in the left ventricular apex is present. Thrombus overlies the thickened endocardium (arrows). |
already received cancer therapy, echocardiography is useful to evaluate for side effects. Adriamycin, for example, can cause cardiomyopathy. Chest irradiation can result in constrictive pericarditis or scarring and fibrosis of the epicardial coronary arteries. In unstable or critically ill patients, the portability and noninvasive nature of ultrasound represent a significant advantage.
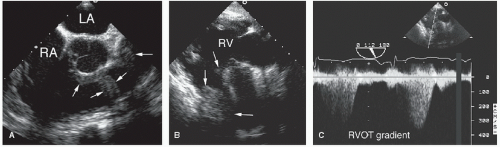 FIGURE 23.15. A primary fibrosarcoma is demonstrated in the right side of the heart. A: The tumor involves the right ventricular outflow tract and pulmonary artery. B: Narrowing of the right ventricular outflow tract is indicated by the arrows. C: Doppler imaging demonstrates a right ventricular outflow tract gradient of approximately 50 mm Hg. |
 FIGURE 23.16. A large sarcoma is shown involving the right atrium (black arrows) and left atrium (white arrowhead). Note how the invasive tumor restricts the normal motion of the heart on real-time imaging. |
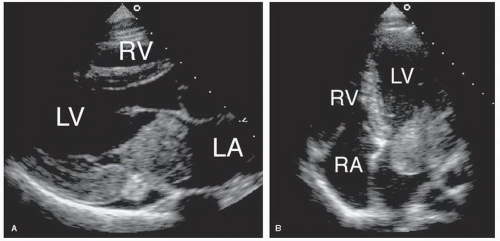 FIGURE 23.17. A, B: An example of angiosarcoma. The mass had infiltrated the lateral wall of the left atrium and left ventricle and invaded the mitral valve. Obstruction to mitral inflow was present. In real time, the heart appeared fixed due to infiltration by the malignancy. A pericardial effusion is also present. |
Table 23.4 Metastatic Tumors to the Heart: Source and Cardiac Manifestations | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
 FIGURE 23.18. Metastatic melanoma often involves the heart. A: Image quality prevents visualization of the apical mass. B: After contrast injection, the outline of the apical mass (arrows) is apparent. |
formation of a pseudoaneurysm that gradually increased in size until the time of the patient’s death. Intramyocardial involvement is less common than pericardial metastases and usually occurs secondary to lymphoma or melanoma. Heart failure, obstruction to flow, and arrhythmias may develop as a result. Cardiac involvement is often established at autopsy as an incidental finding in patients with widely metastatic disease. Figure 23.22 is taken from a patient undergoing treatment of a B-cell lymphoma. The tumor had spread to the heart and can be seen filling the right atrium and extending into the left atrium. Figure 23.23 is an example of a pericardial mesothelioma. The mass is huge and grossly distorts the right side of the heart. Figure 23.24 shows a patient with lymphoma, before and after chemotherapy. The tumor involved the aortic root and posterior wall of the heart, including the area of the coronary sinus. After successful chemotherapy, normal anatomy is restored. In this case, serial echocardiography was critical to follow the progress of therapy and the reduction in tumor burden.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


