Despite advances in antibiotic therapy and surgical options, infective endocarditis remains a challenging and often fatal condition. One reason for this is the difficulty of establishing an accurate diagnosis, particularly early in the course of the disease when proper management can be lifesaving. As therapeutic approaches have become more successful, the importance of early and accurate diagnosis is self-evident. Unfortunately, no single test or finding establishes the diagnosis in all cases. Instead, a constellation of findings that constitutes the diagnostic criteria continues to evolve.
The central role that echocardiography plays in the diagnosis of endocarditis began in the early 1970s with the echocardiographic demonstration of a valvular vegetation by the M-mode technique. With the advent of two-dimensional and Doppler modalities, echocardiography has become virtually indispensable in the diagnosis and management of these patients. Today, echocardiographic findings are a central part of the diagnostic criteria for infective endocarditis.
Clinical Perspective
Infective endocarditis is defined as a localized infection anywhere on the endocardium, including the chamber walls, vessels, and within congenital defects. The vast majority of vegetations, however, occur on valve leaflets. Infection may also develop on any implanted or prosthetic material such as prosthetic valves, conduits, pacing electrodes, and catheters. In recent years, the importance of intracardiac devices as a risk factor for the development of endocarditis has increased. As the proliferation of such devices increases, especially in older and sicker patients, the incidence of infection in this setting will further rise. The process of developing endocarditis occurs in the setting of bacteremia or fungemia. The initiating event usually requires the presence of a high-velocity jet, which may be due to a congenital anomaly such as a ventricular septal defect, a regurgitant valve, or a prosthetic valve. It is thought that the jet interferes with the protective endothelial surface, allowing the blood-borne pathogens to adhere and coalesce. As the nidus of infection organizes, masses of microorganisms attract platelets, fibrin, and other material and become adherent to the endothelial surface to form a vegetation. The vegetation will grow in size, either as a sessile clump or as a highly mobile and even pedunculated mass with the potential for embolization. As the hallmark of endocarditis, the ability to detect the vegetation is the focal point of diagnosis. This sequence of events offers a mechanism for development of endocarditis in patients with underlying heart disease. However, since as many as 50% of patients who get endocarditis do not have lesions associated with a high-velocity jet, some other set of conditions must be operational in these patients to explain the link between bacteremia and cardiac involvement.
Thus, the classic approach to the diagnosis of endocarditis, developed by von Reyn and colleagues in the early 1980s, focused on pathologic evidence of infection within the heart and relied heavily on the presence of positive blood cultures for an appropriate organism in association with clinical evidence suggesting endocarditis. This initial series included 123 cases diagnosed using strict clinical criteria (von Reyn et al., 1981). The von Reyn criteria quickly became the standard by which the diagnosis of endocarditis was established. Because “probable” endocarditis required confirmatory clinical evidence, early or less severe forms of the disease were not included. Importantly, the von Reyn definitions did not include echocardiographic findings as part of the criteria.
Echocardiographic Characteristics of Vegetation
The versatility of echocardiography in the evaluation of endocarditis is illustrated in Table 14.1. Among its important functions is the identification of underlying heart disease known to increase a patient’s risk of infection. Although the absence of underlying disease does not confer protection against endocarditis, particular conditions, such as congenital heart disease and a myxomatous mitral valve, are known risk factors. At the same time, these conditions often confound the diagnosis of endocarditis by creating abnormalities that mimic or conceal echocardiographic evidence of infection.
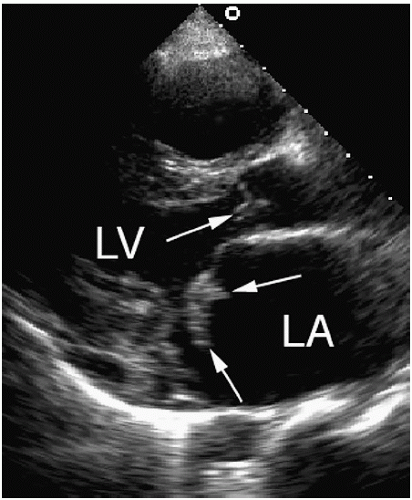
An essential first step in the echocardiographic evaluation is to search for evidence of acute ongoing infection. Although there are several manifestations of endocarditis, including abscesses and fistulae, the most common and direct evidence of infective endocarditis is the vegetation. Because a vegetation begins as a microscopic focus of infection and gradually grows into a conspicuous mass, its presence may or may not be evident on an imaging study. Thus, echocardiography must be sensitive enough to detect the vegetation and specific enough to distinguish it from other echocardiographic abnormalities or artifacts. As can be seen in Table 14.2, certain echocardiographic features can be used to either increase or decrease the probability that a mass is due to endocarditis, that is, represents a vegetation. A vegetation is typically an irregularly shaped, highly mobile mass attached to the free edge of a valve leaflet. Vegetations tend to develop on the upstream side of the valve, that is, the ventricular side of the aortic valve and the atrial side of the mitral valve (Fig. 14.1). They may be sessile or pedunculated but usually have motion that is independent of the valve itself. Because they often occur in the path of a high-velocity jet, their motion is frequently described as oscillating or fluttering. The presence of significant mobility, or oscillating motion, is a classic feature of most vegetations. In fact, the absence of mobility argues against the diagnosis and should suggest the possibility of an alternative diagnosis. The shape and size of vegetations are quite variable and may either increase (due to progression of disease) or decrease (due to healing or embolization) over time. Fungal vegetations tend to be larger than those caused by bacterial infections, and those involving the tricuspid valve tend to be larger compared with vegetations that affect the aortic or mitral valve.
Table 14.1 Role of Echocardiography in Patients with Endocarditis
Identifies predisposing heart disease
Pivotal role in diagnosis
Detects complications
Assesses hemodynamic consequences
Serial evaluation (assesses efficacy of therapy)
Prognosis (risk of complications)
Table 14.2 Echocardiographic Criteria for Defining a Vegetation
Positive Feature
Negative Feature
Low reflectance
High echogenicity
Attached to valve, upstream side
Nonvalvular location
Irregular shape, amorphous
Smooth surface or fibrillar
Mobile, oscillating
Nonmobile
Associated tissue changes, valvular regurgitation
Absence of regurgitation
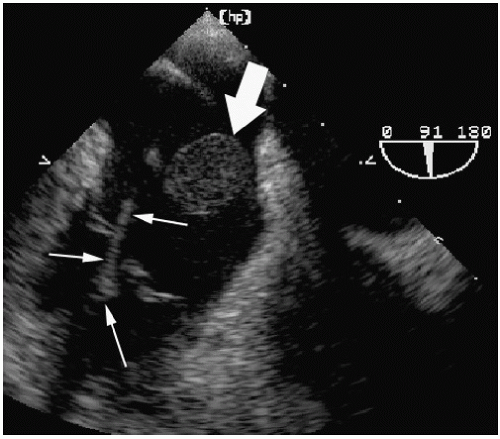
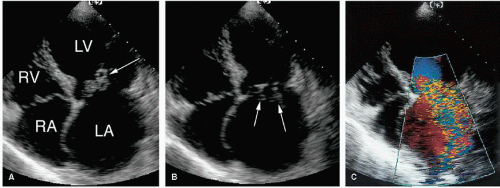
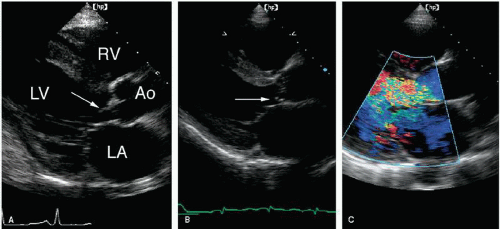
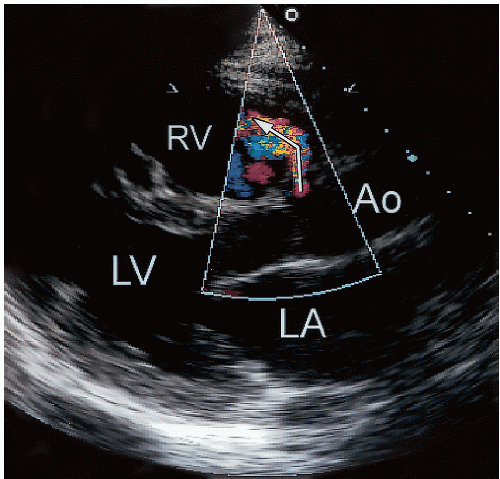
Although typically attached to a valve, vegetations may also attach to chordae, chamber walls, or any foreign body, such as a pacemaker lead, indwelling catheter, and prosthetic valve sewing ring. Figure 14.2 is an example of endocarditis involving a porcine tricuspid valve as well as the pacing wire that extends through it. The mass itself is typically homogeneous with echogenicity similar to that of the myocardium. However, vegetations can occasionally be cystic or appear more dense and calcified. The infectious process often alters valve structure and function. As a result, some degree of regurgitation is associated with most cases of acute endocarditis. In Figure 14.3, a patient with a mitral valve vegetation is shown. The involvement is extensive, and the valve appears partially flail. There is severe mitral regurgitation. A patient with significant aortic regurgitation associated with an aortic valve vegetation is shown in Figure 14.4. Although the vegetation does not appear to be large, its effect on valve function is evident. If the process results in destruction of underlying tissue leading to a flail or perforated valve structure, the degree of regurgitation will be severe. For example, if the infection leads to mitral chordal rupture, severe mitral regurgitation will ensue. This is demonstrated in Figure 14.5, taken from a patient with a flail mitral valve in the setting of staphylococcal endocarditis. Figure 14.6 is an example of a small perforation of the noncoronary cusp of the aortic valve due to infection. Mild aortic regurgitation was present, but no definite vegetation was identified. Much less often, a large vegetation will obstruct the valve orifice, leading to a functional form of valve stenosis (Fig. 14.7).
FIGURE 14.1. An example of vegetations involving the mitral and aortic valves. The vegetations are indicated by the arrows.
FIGURE 14.2. Transesophageal echocardiography shows a large mass (large arrow) attached to a pacemaker lead (small arrows) in the right atrium. This mass most likely represents an infected thrombus.
Although most vegetations involve the valves, in some cases the infection may extend to other structures, such as the chamber wall. Figure 14.8 shows an unusual vegetation attached to the posterior wall of the left atrium, near the base of the posterior mitral leaflet. The three-dimensional echocardiogram shows a small sessile mass protruding from the wall of the chamber (and is best appreciated by viewing the video loop). Another example of this manifestation of infection is shown in Figure 14.9. In this case, the vegetation adhered to the wall of the left atrium and the posterior mitral valve annulus.
It should be emphasized that there is no single characteristic on the echocardiogram that will conclusively identify a mass as a vegetation. The ability to detect a vegetation depends on vegetation size, location, the presence of underlying heart disease, image quality, and instrument settings. All available echocardiographic windows should be used, and Doppler flow mapping should be performed to identify any associated valvular regurgitation. Although masses as small as 2 mm have been reported, in most cases, a vegetation must be at least 3 to 6 mm in size to be reliably seen. Image quality will also influence our ability to visualize small structures. As is discussed later, these are areas in which the advantages of transesophageal echocardiography have been demonstrated.
To avoid false-positive results, vegetations must be differentiated from other echo-producing abnormalities, such as myxomatous processes, degenerative changes (including Lambl’s excrescences and calcification), tumors, thrombi, and imaging artifacts. Figure 14.10 is taken from a patient who was asymptomatic. The large mitral valve mass could easily be mistaken for a vegetation. However, the absence of clinical signs of infection suggests an alternative diagnosis. In this case, the mass was a blood cyst. Underlying heart disease both obscures the presence of a vegetation and increases the likelihood of false-positive findings through misinterpretation (Fig. 14.11). Thus, the accuracy of echocardiography is greater in patients without underlying valve disease. Furthermore, active vegetations must be differentiated from old or healed vegetations. Some studies have suggested that vegetations tend to become smaller and more circumscribed and echogenic over time as part of the healing process. Although this is generally true, a reduction in vegetation size might also suggest embolization. Thus, distinguishing active from healed vegetations can never rely on echocardiography alone but must take into account clinical factors.
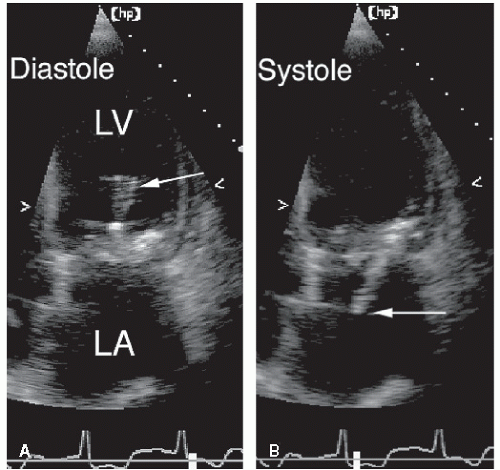
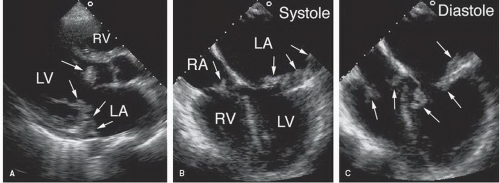
FIGURE 14.3. A large vegetation involving the anterior mitral leaflet. A: The size and location of the mass is evident (arrow). B: During systole, the vegetation can be seen on the left atrial side of the mitral valve (arrows). C: Color Doppler imaging reveals severe mitral regurgitation.
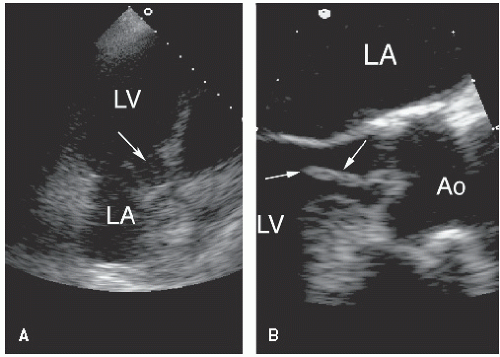
FIGURE 14.4. A small aortic valve vegetation (arrow) is shown during diastole (A) and systole (B). C: Color Doppler imaging demonstrates severe aortic regurgitation.
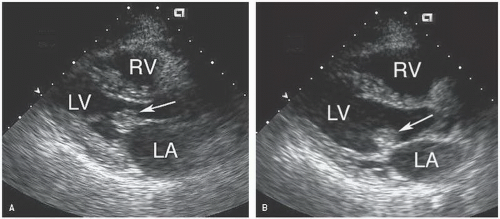
FIGURE 14.5. Extensive infection involving the mitral valve. A: A diastolic frame demonstrates an elongated highly mobile mass (arrow) within the left ventricle. B: During systole, the mass extended through the mitral orifice into the left atrium (arrow). The infectious process had destroyed part of the valve structure resulting in severe regurgitation.
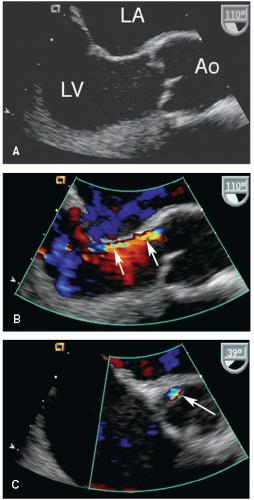
FIGURE 14.6. A transesophageal echocardiogram demonstrates a small perforation of the noncoronary cusp of the aortic valve. A: Focal thickening is seen but no definite vegetation. B: Color Doppler imaging demonstrates the jet extending through the cusp (arrows). C: A short-axis view confirms the location of the perforation (arrow).
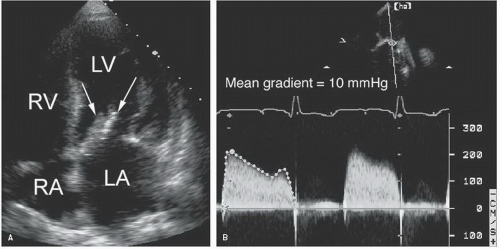
FIGURE 14.7. A: A large vegetation involving the anterior mitral leaflet (arrows). B: Spectral Doppler imaging recorded a 10 mm Hg mean gradient across the mitral valve.
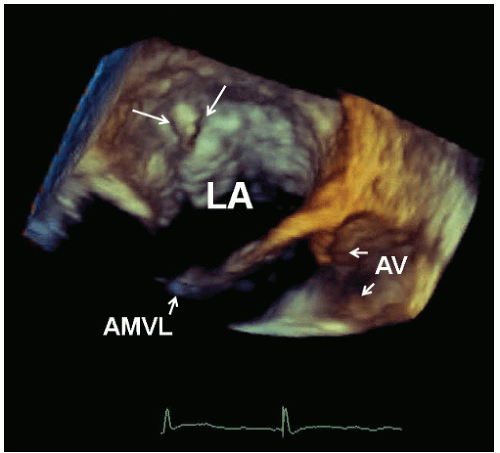
FIGURE 14.8. An unusual vegetation (arrows) is shown attached to the wall of the left atrium and best visualized with three-dimensional transesophageal echocardiography. The mobile mass arises from the atrial wall just behind the posterior mitral leaflet. The patient also had endocarditis involving the right heart. AMVL, anterior mitral valve leaflet; AV, aortic valve.
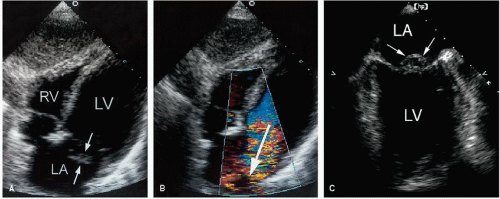
FIGURE 14.9. A: The arrows indicate multiple masses within the left ventricle and left atrium, consistent with vegetations. Transesophageal echocardiography confirmed these findings and also revealed involvement of the tricuspid valve (arrows). B: Note the location of the mass within the left atrium, extending from the base of the mitral leaflet along the wall of the left atrium (arrows). C: A diastolic frame demonstrates the highly mobile nature of the vegetations (arrows).
FIGURE 14.10. An example of a blood cyst (arrow) is demonstrated within the mitral valve. Diastolic (A) and systolic (B) frames are shown. Such an appearance could easily be confused with vegetation.
FIGURE 14.11. This echocardiogram was recorded from a patient with mitral valve prolapse and significant mitral regurgitation. The mitral valve was myxomatous and partially flail. A: The prolapsing valve is indicated by the arrows.B: Severe mitral regurgitation is demonstrated (arrow). C: A transesophageal echocardiogram demonstrates the prolapsing scallop (arrows). This could easily be mistaken for a vegetation.
Diagnostic Accuracy of Echocardiography
Over the past 30 years, numerous clinical studies have tested the accuracy of echocardiography to detect vegetations and other manifestations of acute endocarditis. A limitation of all these studies is the difficulty in defining the standard by which the diagnosis is established. In most series, a clinical standard for diagnosis was used that incorporated clinical findings, blood culture results, response to therapy, and outcome measures. Although practical, this approach has obvious limitations and very likely permitted the inclusion of some patients who had bacteremia but never had endocarditis. More rigorous diagnostic standards that required pathologic and/or surgical confirmation must, by definition, exclude patients who have endocarditis but never come to either surgery or autopsy. As a result, only the “sickest of the sick” would be included in such series. Finally, the recognition over time of the fundamental involvement of echocardiography in establishing a diagnosis made it increasingly difficult to “test the test.” That is, it becomes impossible to establish the accuracy of a test (in this case, echocardiography) that is fundamentally involved in the definition of disease. For all these reasons, the exact sensitivity and specificity of the various echocardiographic techniques must be interpreted in context. Despite these limitations, the overall utility of echocardiography as an integral part of the diagnostic algorithm is well established.
A summary of the studies examining transthoracic echocardiography for the diagnosis of endocarditis is presented in Table 14.3. The sensitivity of the transthoracic technique to detect vegetations is 60% to 70%. Size and image quality are clear determinants of the ability of echocardiography to detect a vegetation. Using the transthoracic approach, sensitivity for the detection of endocarditis in patients with prosthetic valves is significantly lower, as is discussed later. It should be recognized that some patients with endocarditis may not have vegetations, thereby accounting for some false-negative results. Establishing the specificity of the technique is more difficult. Although the reported false-positive rate is quite low in most series, specificity will vary widely depending on the population being studied and the criteria used to define disease. As previously discussed, distinguishing active vegetations from healed vegetations, myxomatous change, or tumors in the absence of clinical information is nearly impossible. In most cases, echocardiography is interpreted in context, thereby avoiding most false-positive results.
Table 14.3 Diagnostic Accuracy of Echocardiography for Detecting Endocarditis
Sensitivity (%)
Reference
N
TTE
TEE
Erbel et al., 1988
166
63
100
Mugge et al., 1989
91
58
90
Shively et al., 1991
66
44
94
Birmingham et al., 1992
63
30
88
Shapiro et al., 1994
64
68
91
Lowry et al., 1994
93
36
93
Werner et al., 1996
104
60
93
TEE, transesophageal echocardiography; TTE, transthoracic echocardiography.
FIGURE 14.12. This aortic valve vegetation was not detected on transthoracic imaging (A). The arrow points toward the aortic valve, but the mass was not visualized. B: The transesophageal echocardiogram clearly demonstrates the vegetation.
Beginning in the mid-1980s, the potential advantages of transesophageal echocardiography in assessing patients with suspected endocarditis were first recognized. As is apparent in Table 14.3, the sensitivity of transesophageal echocardiography is consistently higher than that of the transthoracic technique. The improved image quality and the closer proximity between transducer and valves account for much of this difference. Smaller vegetations, those associated with prosthetic valves, and those in locations that would be shadowed or obscured during transthoracic scanning are some of the areas in which the transesophageal approach is superior.
When the two echocardiographic techniques are compared in the same patient population, the superior sensitivity of transesophageal imaging has been a consistent finding (Fig. 14.12). At the same time, many of these contemporary series have reported a sensitivity of transthoracic echocardiography that is lower than would be otherwise expected. This may be partly explained by the mere availability of transesophageal imaging. If the transthoracic examination is approached with less determination and rigor, small lesions may be missed, thereby contributing to the wide difference in sensitivity between the two tests. Although the superiority of the transesophageal approach is beyond question, the magnitude of the difference (i.e., the surprisingly low sensitivity of transthoracic echocardiography) is noteworthy. Some of this may be explained on the basis of patient selection that included a greater percentage of individuals with a relatively low pretest likelihood of disease. Alternatively, the availability of transesophageal echocardiography may have indirectly contributed to the performance of a more cursory and less rigorous transthoracic study, followed by a thorough and complete transesophageal examination. An additional advantage of transesophageal echocardiography is its ability to identify other manifestations of endocarditis, such as ring abscesses and fistulae (Fig. 14.13). Despite the relatively modest sensitivity of transthoracic echocardiography, a normal study in the presence of excellent image quality is strong evidence against endocarditis.
The impact of three-dimensional echocardiography in this area is still undefined. Figure 14.14 is an example of an aortic valve vegetation recorded with three-dimensional imaging. In theory, the ability of three-dimensional echocardiography to visualize an entire valve (rather than individual slices of the valve) should improve sensitivity by reducing false-negative results. Unfortunately, most missed echocardiographic diagnoses are related to image quality, which would also negatively affect three-dimensional images. That is, if a vegetation is missed on two-dimensional imaging because of poor image quality, it may not be seen on three-dimensional imaging for the same reason.
FIGURE 14.13. A fistula between the left ventricular outflow tract and the right ventricle (arrow) is demonstrated from this transthoracic echocardiogram using color Doppler imaging. This developed as a complication of an aortic ring abscess.
Image quality is generally not a problem with transesophageal echocardiography, but the high accuracy of twodimensional transesophageal echocardiography will make it difficult for three-dimensional transesophageal echocardiography to demonstrate incremental value. One potential advantage of three-dimensional imaging is the opportunity to obtain a complete visualization of complex cases and provide true spatial assessment of the extent of disease. Much more experience in this area can be expected over the next several years.
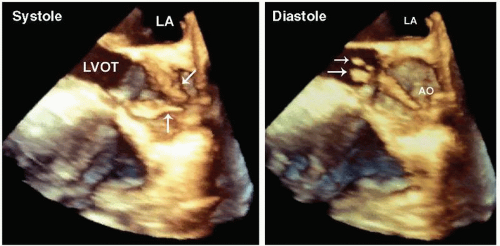
FIGURE 14.14. A vegetation involving a congenitally stenotic aortic valve is demonstrated on three-dimensional transesophageal echocardiography. Left panel: In systole, a doming of the valve cusps is demonstrated. Right panel: In diastole, a mobile mass (arrows) is seen protruding into the left ventricular outflow tract.
Table 14.4 Comparison of von Reyn and Duke Criteria for Diagnosing Endocarditis
von Reyn Definitions
Duke Definitions
Probable
Possible
Rejected
Total (%)
Definite
65
59
11
40
Possible
6
56
87
44
Rejected
0
0
52
15
Total
21%
34%
45%
100
From Durack DT, Lukes AS, Bright DK. New criteria for diagnosis of infective endocarditis: utilization of specific echocardiographic findings. Am J Med 1994;96:200-209, with permission.
Evolution of the Diagnostic Criteria
The clinical diagnosis of infective endocarditis has always been challenging. Before the routine use of echocardiography, establishing the diagnosis of endocarditis focused on evidence of ongoing infection within the blood coupled with clinical evidence of cardiac involvement. In 1994, the Duke Endocarditis Service published new criteria for the diagnosis of endocarditis that relied heavily on echocardiographic findings. In this original study, 405 cases were retrospectively reviewed and classified as definite, possible, or rejected on the basis of the presence or absence of major and minor criteria. When compared with previously used criteria, the newly proposed Duke criteria classified significantly more cases as definite endocarditis. Among pathologically proven cases, the Duke criteria were significantly more sensitive (80%) compared with the von Reyn criteria (51%) (Table 14.4).
Although the original criteria were generally accepted as an important advance in the diagnosis of endocarditis, there were limitations that were addressed in a subsequent publication (Li et al., 2000). Table 14.5 contains the detailed description of terms used to define major and minor criteria, according to the updated modifications. Using these terms, the diagnosis of endocarditis can be confirmed or rejected as described in Table 14.6. On the basis of the four major and five minor criteria, patients can be classified as having definite evidence of endocarditis, possible endocarditis, or the diagnosis can be rejected. This approach has subsequently been endorsed by the American College of Cardiology/American Heart Association practice guidelines for the management of patients with valvular heart disease (Bonow et al., 2006).
Table 14.5 Definition of Terms Used in the Duke Criteria
Major criteria
(1) Blood culture positive for IE
Typical microorganisms consistent with IE from two separate blood cultures:
Viridans streptococci, Streptococcus bovis, HACEK group, Staphylococcus aureus; or
Community-acquired enterococci, in the absence of a primary focus; or
Microorganisms consistent with IE from persistently positive blood cultures, defined as follows:
At least two positive cultures of blood samples drawn >12 hr apart; or
All three or a majority of ≥4 separate cultures of blood (with first and last sample drawn at least 1 hr apart)
Single positive blood culture for Coxiella burnetii or antiphase I IgG antibody titer > 1:800
(2) Evidence of endocardial involvement
(3) Echocardiogram positive for IE, defined as follows:
Oscillating intracardiac mass on valve or supporting structures, in the path of regurgitant jets, or on implanted material in the absence of an alternative anatomic explanation; or
Abscess; or
New partial dehiscence of prosthetic valve
(4) New valvular regurgitation (worsening or changing of preexisting murmur not sufficient)
Minor criteria
(1) Predisposition, predisposing heart condition, or injection drug use
(2) Fever, temperature >38°C
(3) Vascular phenomena, major arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhages, and Janeway lesions
(5) Microbiological evidence: positive blood culture but does not meet a major criterion as noted abovea, or serological evidence of active infection with organism consistent with IE
(6) Echocardiographic minor criteria eliminated
a Excludes single positive cultures for coagulase-negative staphylococci and organisms that do not cause endocarditis.
IE, infective endocarditis.
Adapted from Li JS, Sexton DJ, Mick N, et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis.
Clin Infect Dis 2000;30:633-638.
Only gold members can continue reading. Log In or Register to continue