Table 22.1 Use of Echocardiography in the Intensive Care Unit | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 22.2 Appropriateness Criteria for Transthoracic and Transesophageal Echocardiography | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||
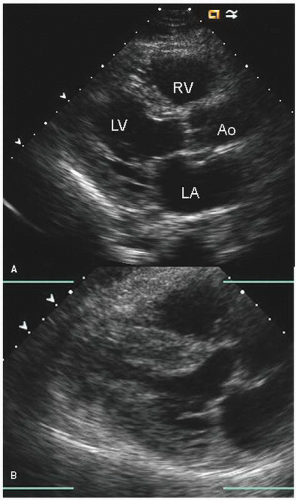 FIGURE 22.1. Parasternal long-axis view recorded in a 42-year-old patient with shock related to gram-negative sepsis. The two views were recorded at end-systole. Notice at the time of presentation (A) the mildly dilated, hypokinetic left ventricle compared to normal ventricular size and function 5 days later, after successful treatment of sepsis (B). |
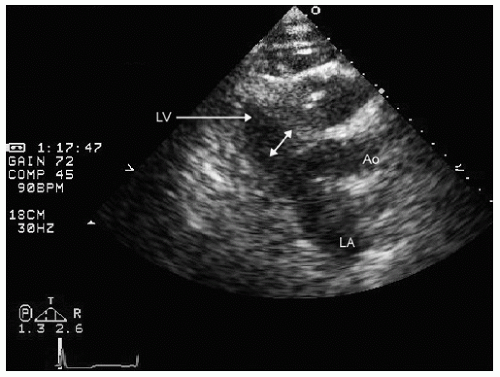 FIGURE 22.2. Parasternal long-axis view recorded in an elderly patient with pneumonia who presented with hypotension and shock. Note the very small left ventricular cavity (double-headed arrow) with normal systolic function suggesting that hypovolemia is the etiology for hypotension. |
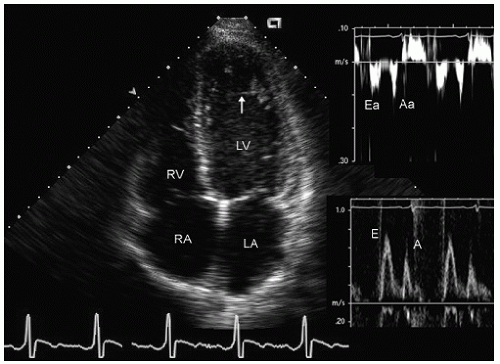 FIGURE 22.3. Apical four-chamber view recorded in a patient with hypotension and shock after an acute febrile illness. Note the global hypokinesis of the left ventricle (consistent with an underlying cardiomyopathy). The Doppler pattern suggests pseudonormal filling (grade 2 diastolic dysfunction). In this instance, there was no recovery of function with treatment of the underlying illness. Incidental note is made of a pseudochord in the left ventricular apex (arrow). |
hypotension in whom the use of intravenous pressors results in no improvement or further deterioration. There is a subset of patients, many of whom have a history of hypertension, who with volume depletion develop acquired dynamic left ventricular outflow tract obstruction which mimics obstructive hypertrophic cardiomyopathy. Systolic anterior motion of the mitral valve with secondary mitral regurgitation also may be seen. The overall hemodynamic result of this syndrome is progressive hypotension with the development of a prominent systolic murmur (due to outflow tract obstruction and/or mitral regurgitation). The etiology of the hypotension in this situation is the relatively low left ventricular stroke volume due to hypovolemia, complicated by outflow tract obstruction. Left ventricular outflow tract gradients exceeding 100 mm Hg have been noted because of this phenomenon. In this instance, right heart catheterization reveals an elevated pulmonary capillary wedge pressure that is then assumed to reflect left ventricular filling volume. When the syndrome of significant mitral regurgitation with outflow tract obstruction is identified, one should recognize that the elevated pulmonary capillary wedge pressure is the result of a hyperdynamic but noncompliant left ventricle and mitral regurgitation. Failure to appreciate this phenomenon results in the inappropriate course of increasing pressor support and diuretics, which obviously has the effect of worsening rather than improving the clinical situation. Figure 22.8 was recorded in a patient with this syndrome. Recognition of hypovolemia with dynamic outflow tract obstruction should lead to the appropriate management decision to resuscitate the patient with fluids and withdraw agents, which increase contractility and/or reduce vascular resistance.
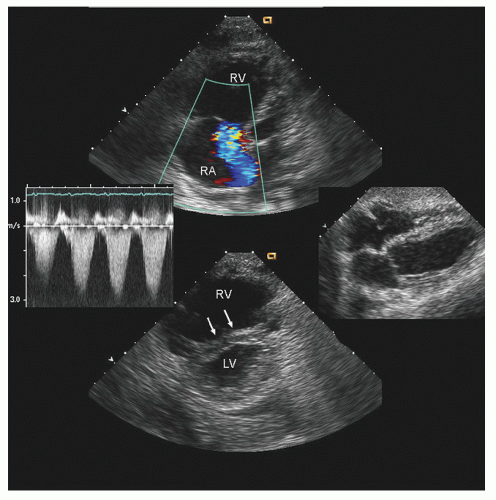 FIGURE 22.4. Transthoracic echocardiogram recorded in a patient with multilobar pneumonia. The middle right figure was recorded 1 year previously and demonstrates normal left and right ventricular size and function. At the time of presentation with hypoxia and multilobar pneumonia requiring mechanical ventilation, note the dilation of the right atrium and right ventricle with a right ventricular overload pattern on the ventricular septum. The tricuspid regurgitation velocity is mildly elevated at 3 m/sec, in line with secondary pressure elevation in a non-preconditioned ventricle. |
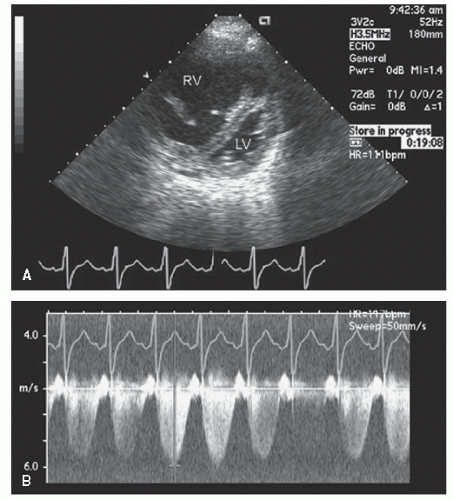 FIGURE 22.5. Parasternal short-axis view recorded in a 37-year-old woman presenting with a febrile illness and hypotension. Note the massively dilated and hypertrophied right ventricle and the small slitlike left ventricle consistent with a severe right ventricular pressure overload. The tricuspid regurgitation gradient suggests systemic right ventricular systolic pressure due to previously unrecognized primary pulmonary hypertension. |
elderly and have a history of hypertension. In the operative or postoperative period, overly aggressive fluid resuscitation may result in congestive heart failure. The echocardiogram will typically reveal normal systolic function and left ventricular hypertrophy (Fig. 22.9). Mitral inflow patterns may be highly variable and show either delayed relaxation or a restrictive filling pattern. If intravascular volume overload is present, a pseudonormal inflow pattern is not uncommon.
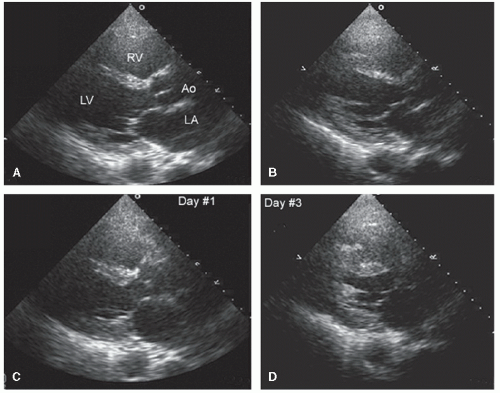 FIGURE 22.6. Serial parasternal long-axis echocardiograms recorded in a 23-year-old patient 4 hours after renal transplantation who developed hypotension and was unable to be weaned from the ventilator. For each pair of images diastole is on the top and systole is on the bottom. A, C: Images recorded at the time of clinical deterioration reveal septal akinesis with otherwise global hypokinesis. B, D: Images recorded 2 days later demonstrate complete recovery of function. In this instance, the left ventricular dysfunction was due to myocardial stunning of uncertain provocation which was not related to obstructive coronary disease. |
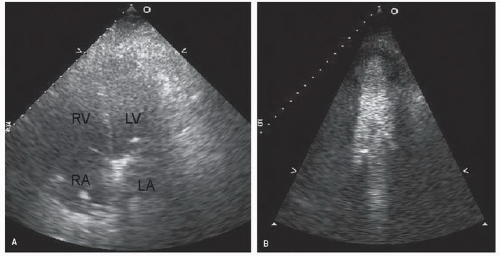 FIGURE 22.7. Apical four-chamber view recorded in a patient hospitalized in a medical intensive care unit with sepsis and multiorgan system failure. A: An apical four-chamber view from which an accurate assessment of left ventricular function cannot be made. B: Recorded after an injection of intravenous contrast for left ventricular opacification, after which normal left ventricular systolic function is noted. |
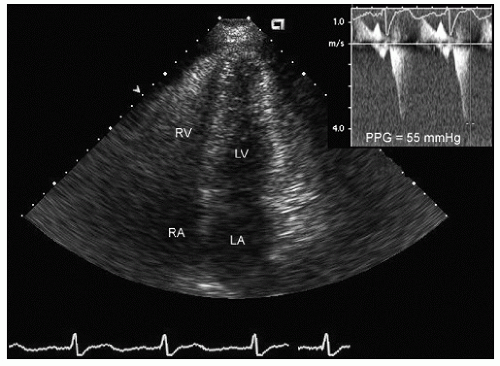 FIGURE 22.8. Apical four-chamber view (end-systolic) recorded in a 60-year-old patient with a gastrointestinal bleed and hypotension. Note the small hyperdynamic left ventricle with midcavity obliteration. Continuous wave Doppler image revealed a midcavity gradient of 55 mm Hg. In this instance, the obstruction is related to hypovolemia and a heightened adrenergic state on the background of hypertension and left ventricular hypertrophy, rather than hypertrophic cardiomyopathy. |
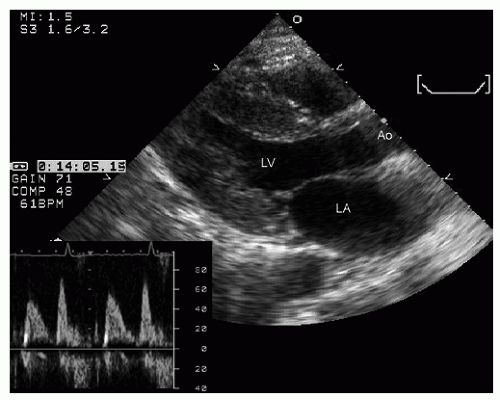 FIGURE 22.9. Parasternal long-axis echocardiogram recorded in a 50-year-old patient with long-standing hypertension admitted to an intensive care unit with ketoacidosis. Note the left ventricular hypertrophy and normal systolic function in this end-systolic image. The accompanying Doppler profile confirms the presence of diastolic dysfunction, which may make this patient susceptible to pulmonary congestion during aggressive volume resuscitation. |
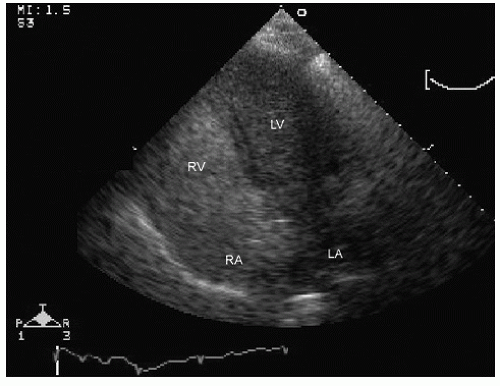 FIGURE 22.10. Apical four-chamber view recorded in a patient with obstructive lung disease and significant hypoxia. Note the significant opacification of the left ventricular cavity after intravenous injection of agitated saline. This is indicative of a significant right-to-left shunt due to opening of a patent foramen ovale. |
with major trauma, hemorrhagic shock is a consideration, in which case echocardiography can quickly document a small, underfilled ventricle. Additionally, in patients with major blunt chest trauma, such as after a high-speed motor vehicle accident, echocardiography can be instrumental in documenting cardiac involvement including myocardial contusion, pericardial effusion, or aortic trauma. By confirming the absence of significant cardiac involvement, echocardiography allows the clinician to redirect efforts to alternate explanations for hypotension.
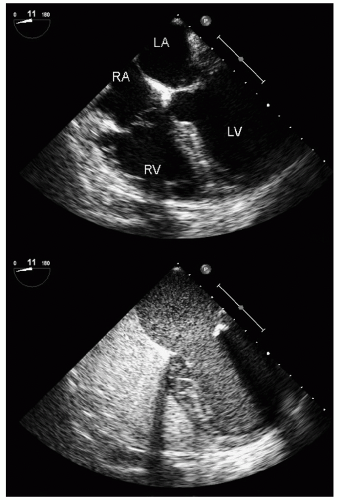 FIGURE 22.11. Apical four-chamber view recorded in a patient with significant hypoxia while on mechanical ventilatory support 24 hours after liver transplantation. In the upper panel, note the mild right heart dilation but the otherwise structurally normal heart and the absence of atrial septal defect. The lower panel was recorded 7 seconds after appearance of intravenous saline in the right side of the heart and demonstrates a substantial right-to-left shunt related to a pulmonary AVM. In the real-time images, note the smooth homogenous buildup of contrast in the left side of the heart, which is a characteristic of a pulmonary AVM, as opposed to phasic appearance typically seen with atrial level shunts. |
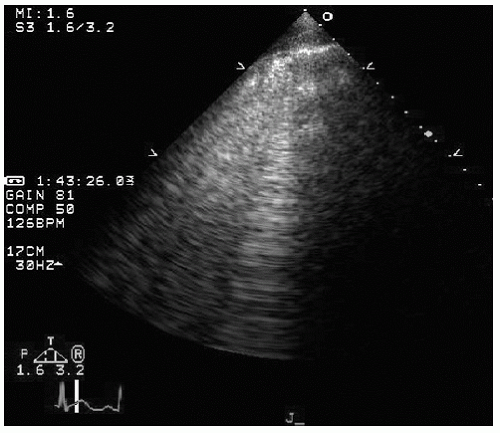 FIGURE 22.12. Attempt to obtain a parasternal long-axis echocardiogram in a patient after a motor vehicle accident. Identical images were obtained from multiple transthoracic transducer positions and reveal only ultrasound “noise.” In the real-time image, notice the oscillating nature of the echoes in the near field. These images are consistent with subcutaneous air secondary to chest trauma. |
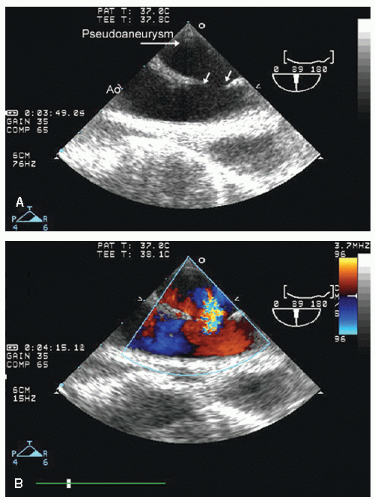 FIGURE 22.13. Transesophageal echocardiogram performed on an emergent basis in a young patient with hypotension, shock, and a left plural effusion after a high-speed motor vehicle accident. The transesophageal echocardiogram identifies a break in the contour of the aorta (arrows) with color flow demonstrating communication between the lumen of the aorta and the extra-aortic space consistent with aortic rupture and pseudoaneurysm. |
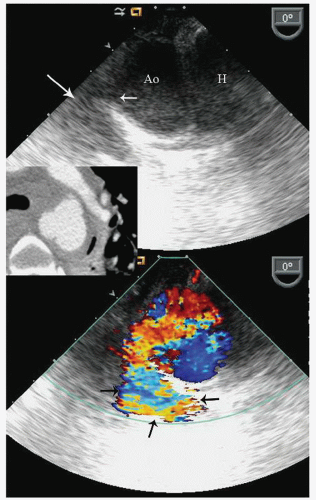 FIGURE 22.14. Transesophageal echocardiogram recorded in a 56-year-old female after a snowmobile accident. The patient presented with thoracic and other trauma with hypotension and shock. The recorded images are at approximately 30 cm from the incisors at the area of the ligamentum arteriosum. Note the break in the aortic wall (small arrow) and the echo-free space adjacent to the aorta (large arrow). Color Doppler image confirmed flow from the aortic lumen into the periaortic space. The inset is a contrast-enhanced computed tomogram at the equivalent level of the aorta, also showing disruption of the aortic contour. |
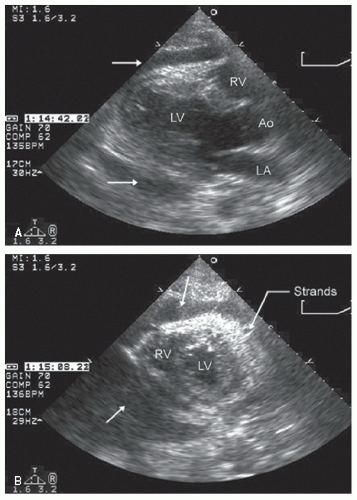 FIGURE 22.15. Parasternal echocardiogram recorded in a patient with hypotension and shock after a gunshot wound to the chest. Note in both the parasternal long-axis and shortaxis views that there is a “cloudy” pericardial effusion (arrows) consistent with acute hemorrhage into the pericardium. In the real-time image, note the apical akinesis consistent with myocardial or coronary arterial injury. There was no evidence of penetration of the heart in this case. |
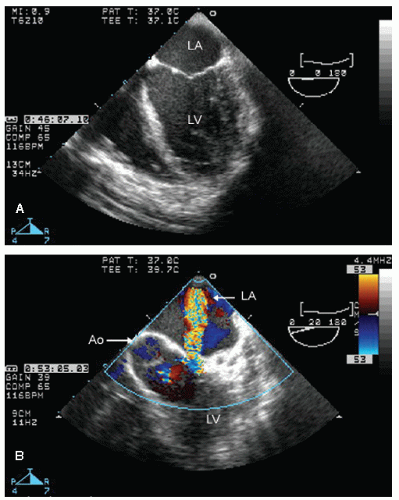 FIGURE 22.16. Transesophageal echocardiogram recorded in a young patient with hypotension, shock, and a loud murmur after a stab wound to the chest. In the longitudinal view, note the global hypokinesis of both the left and right ventricles, the etiology of which is presumed to be coronary injury. Color flow imaging reveals an abnormal communication between the left ventricular cavity and the left atrium consistent with a direct penetrating injury of the mitral valve. |
residual gradients and paravalvular regurgitation. Preoperative echocardiography is instrumental in assessing the indications for, and the likelihood of success of virtually all forms of valve surgery.
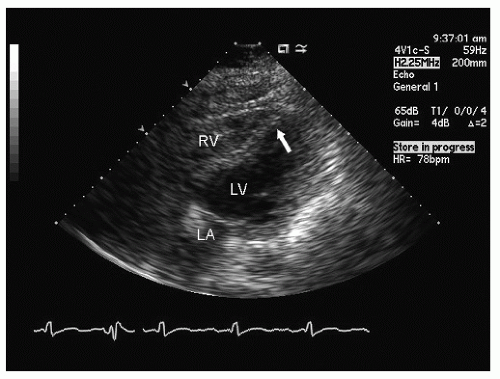 FIGURE 22.17. Subcostal four-chamber view recorded in a 56-year-old male after resuscitation from a witnessed cardiac arrest. In this subcostal view, note the dyskinesis of the apical septum and otherwise globally hyperkinetic ventricle, suggesting ischemic heart disease as the most likely etiology. |
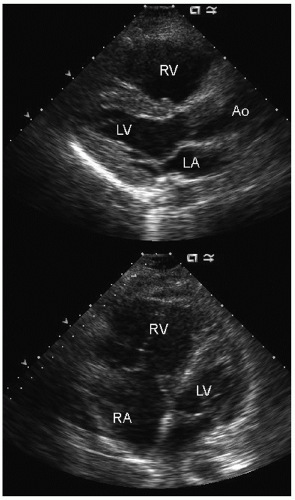 FIGURE 22.18. Echocardiogram recorded in a 32-year-old patient immediately following resuscitation from cardiac arrest characterized as pulseless electrical activity (PEA). Note the marked dilation of the right atrium and ventricle and the small, underfilled left ventricle with normal left ventricular function. This pattern should direct attention toward an acute right ventricular insult such as massive pulmonary embolus, which was the subsequent diagnosis in this patient. |
Table 22.3 Echocardiography in the Operating Room | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
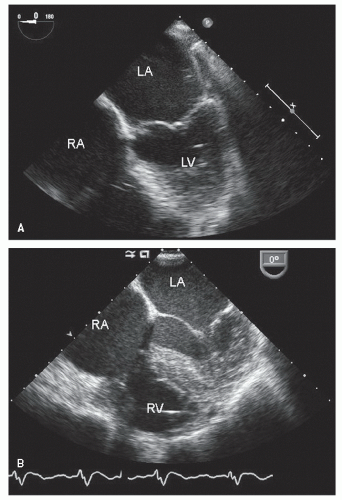 FIGURE 22.19. Transesophageal echocardiogram recorded on an outpatient basis (upper panel) and in the operating room (lower panel) after opening the chest and pericardium but before institution of cardiopulmonary bypass. A: Note the more ideal orientation of the atria as well as the size of the left atrium. B: Recorded at the same plane rotation (0°), note the distortion of atrial anatomy and the less optimal visualization of the plane of the mitral valve, which is the result of the position of the heart within the chest after opening of the pericardium. |
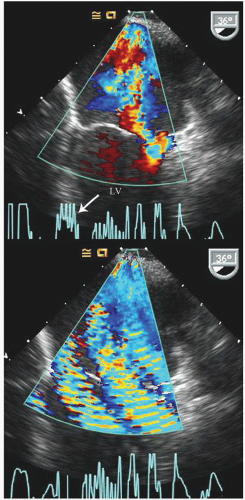 FIGURE 22.20. Intraoperative transesophageal echocardiogram recorded before (upper panel) and during activation of an electrocautery device resulting in substantial distortion of the image, rendering it essentially uninterpretable. Also note the inadequate electrocardiographic signal, further complicated by interference from the electrocautery (arrow). |
even in the beating heart, the ventricle will appear globally hypokinetic (Fig. 22.21). Once fully removed from bypass and after appropriate volume resuscitation, ventricular size and function should return to baseline. Depending on the nature of the surgery and its success, and the use of inotropic agents, ventricular function may be improved compared with baseline. Partial bypass, or incomplete volume restoration, results in intermediate levels of ventricular performance. While on complete bypass, continuous nonphasic flow will be seen in the aorta, related to the cardiopulmonary bypass cannula flow (Fig. 22.22).
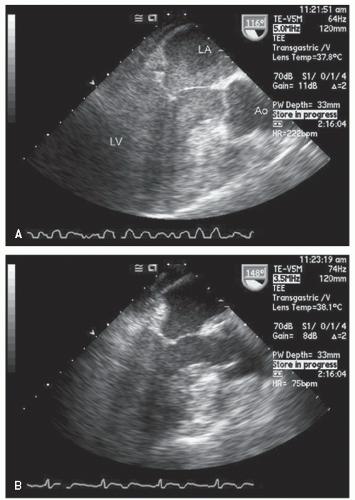 FIGURE 22.21. Transesophageal echocardiograms recorded in a patient on complete (A) and partial (B) cardiopulmonary bypass. A: Note that while on complete bypass, the left atrium and left ventricle are filled with homogeneous echoes consistent with marked stasis of blood flow. Note the fibrillating left ventricle. Also note the relative absence of stasis in the aorta, which receives flow from a cardiopulmonary bypass cannula. B: Recorded after restoration of sinus rhythm and while on partial (1.5 L/min) cardiopulmonary bypass. Again, note the underfilled left ventricle with the poor ventricular function due to reduced filling and the substantial clearing of the spontaneous contrast within the chambers. |
the medial commissures to the right. When viewed with either transesophageal or transthoracic echocardiography, this orientation will be reversed (assuming traditional recommended viewing formats on a video screen). Also, depending on whether the reference is a transthoracic or transesophageal echocardiogram, the anterior and posterior leaflets of the mitral valve will vary in position compared with the surgical perspective.
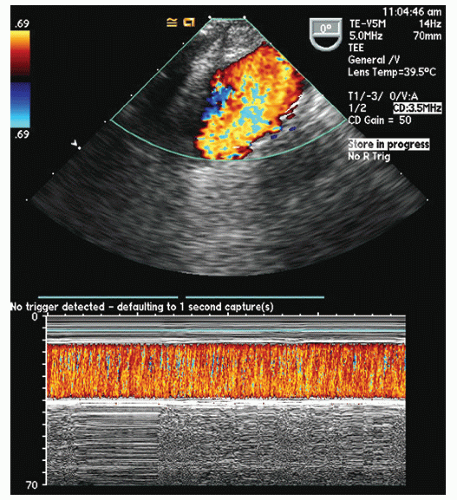 FIGURE 22.22. Intraoperative transesophageal echocardiogram of the aortic arch during cardiopulmonary bypass. Note the continuous high-velocity flow in the aortic arch on the color flow image, which is also appreciated in the color Doppler M-mode image. This is the result of continuous flow into the aorta from the cardiopulmonary bypass apparatus and does not represent pathology. |
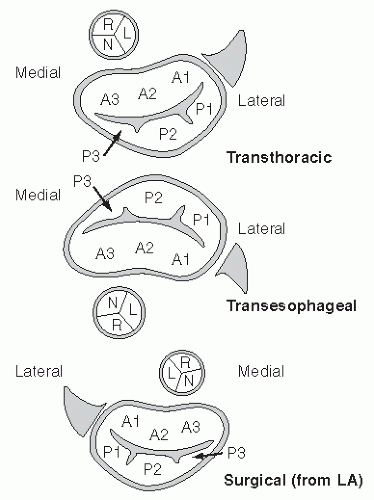 FIGURE 22.23. Schematic of the mitral valve from multiple perspectives. Bottom: The mitral valve from the surgical perspective, from inside the left atrium. Top: The mitral valve as viewed from a traditional transthoracic parasternal short-axis view. Middle: The mitral valve is seen from a transesophageal approach at the midgastric level. In each instance, the proximal aorta is as noted in the schematic, as is the left atrial appendage. The three distinct scallops of the anterior (A1, A2, A3) and posterior (P1, P2, P3) leaflets are also schematized. |
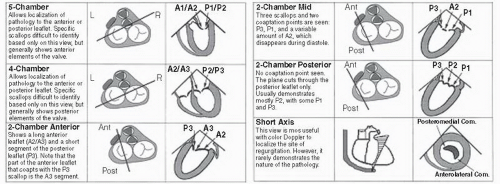 FIGURE 22.24. Summary figure of multiple transesophageal echocardiographic views for visualizing the mitral valve in relation to preoperative planning. A1, A2, A3, anterior scallops; Ant, anterior; P1, Com., commissure; P2, P3, posterior scallops; Post, posterior. (From Lambert AS, Miller JP, Merrick SH, et al. Improved evaluation of the location and mechanism of mitral valve regurgitation with a systematic transesophageal echocardiography examination. Anesth Analg 1999;88:1205-1212, with permission.) |
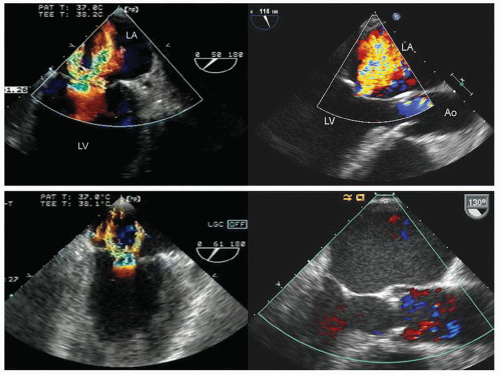 FIGURE 22.25. Transesophageal echocardiograms recorded in two ambulatory outpatients (upper panels) and in the operating room while intubated and under general anesthesia (lower panels). On the left, note the decrease in apparent severity of mitral regurgitation after institution of general anesthesia and on the right, the marked decrease in size of the left ventricular cavity and absence of previously noted moderate mitral regurgitation. |
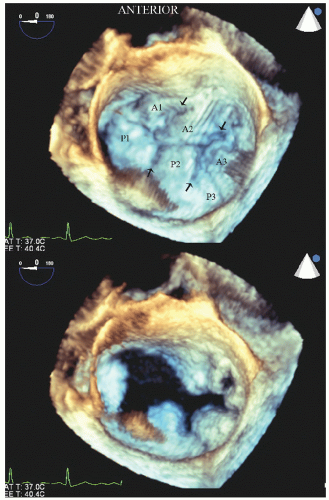 FIGURE 22.26. Real-time three-dimensional transesophageal image recorded in a patient with a myxomatous mitral valve and mitral valve prolapse. Because of the thickened myxomatous leaflets, the individual scallops are easily appreciated. This image is recorded from a “surgical perspective” with the anterior aspect at the top of the image. The individual scallops of the mitral valve are as noted (A1, P1, etc.) and the interscallop commissures also easily visualized (small arrows). |
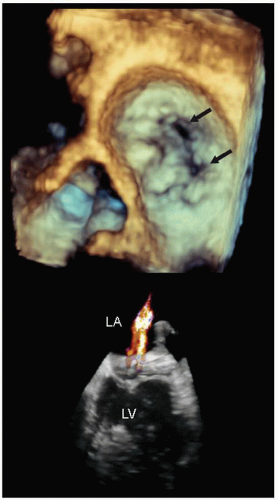 FIGURE 22.27. Real-time three-dimensional echocardiogram recorded from a left atrial perspective in a patient with mitral regurgitation related to ischemic heart disease. The image was recorded in midsystole and two separate regurgitant orifices (arrows) are clearly demonstrated. In the three-dimensional color Doppler image, the two distinct mitral regurgitation jets can be visualized. |
of the mitral valve from a perspective within the left atrium (Fig. 22.26). Experience suggests that real-time three-dimensional imaging confers an advantage with respect to complete evaluation of mitral valve pathology, including isolated mitral flail chordae and precise localization of flail scallops compared with routine, two-dimensional imaging, although the true clinical impact of this has yet to be demonstrated. Figures 22.27, 22.28 and 22.29 were recorded in patients with mitral pathology and demonstrate the unique capabilities of this type of imaging. Similar images can be obtained from reconstructed images but are
limited by artifacts inherent in stitching subvolumes and the fact that they do not provide true real-time images. Sophisticated on- and off-line analysis systems have been developed for quantitation of the three-dimensional mitral valve data set allowing determined quantitation of the actual amount of mitral valve tissue involved with a flail leaflet as well as the overall area of the mitral valve (Fig. 22.29). Experience to date suggests that this imaging technique confers substantial clinical value with respect to accuracy and speed of anatomical diagnosis, both before and following surgery for mitral valve disease. As current ultrasound platforms are still limited with respect to color Doppler imaging when operating in a threedimensional scanning mode, standard two-dimensional imaging with color flow Doppler is still essential for a complete evaluation.
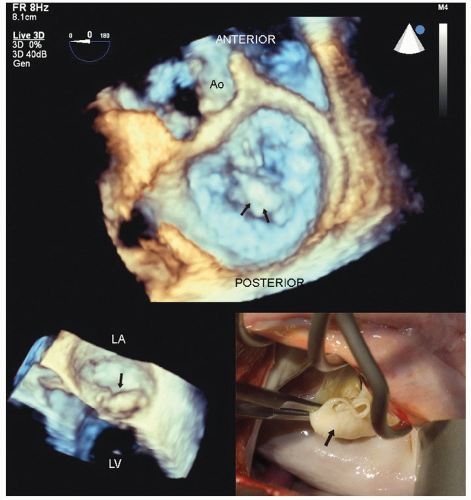 FIGURE 22.28. Real-time three-dimensional transesophageal imaging in a patient with myxomatous mitral valve disease and pronounced buckling of the posterior leaflet. This image was recorded from the perspective of the surgeon’s view within the left atrium. Note the large, bulky myxomatous posterior leaflet protruding into the left atrium in systole (arrows). The smaller inset is a real-time image of the same patient revealing the myxomatous posterior leaflet buckling into the left atrium (arrow). The intraoperative anatomy is also illustrated for comparison (see Figs. 22.35 and 22.36 for the postoperative images). |
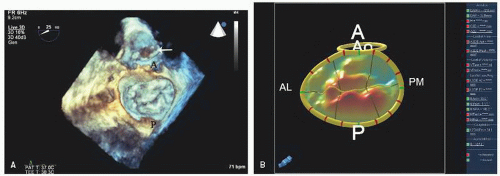 FIGURE 22.29. Real-time three-dimensional transesophageal echocardiogram recorded in a patient with mitral valve prolapse and moderate to severe mitral regurgitation. The viewing prospective is from within the left atrium as viewed from the surgical perspective. A: In this systolic image, note the prolapse of both the anterior and posterior leaflets with more prominent posterior leaflets. B: Computer-generated map of the anterior and posterior mitral leaflets with red areas denoting progressive amounts of prolapse behind the plane of the mitral annulus. A, anterior, AL, anterior lateral; P, posterior, PM, posterior medial. |
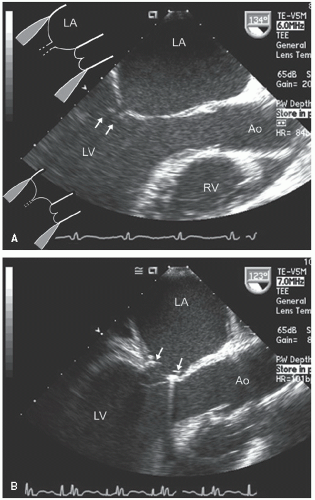 FIGURE 22.30. Pre- and postoperative transesophageal echocardiograms recorded in a patient with left ventricular dysfunction and mitral regurgitation due to failure of mitral valve coaptation. Longitudinal views recorded at end-systole are presented. A: Prerepair, note the apical displacement of the mitral valve tips and the failure to coapt (arrows) in this systolic frame. The schematic in the upper left of (A) depicts the effect of apical and lateral tethering of the papillary muscles with incomplete valve coaptation. Normal coaptation is depicted in the lower schematic. B: Recorded after successful repair by placement of an annular ring (arrows). |
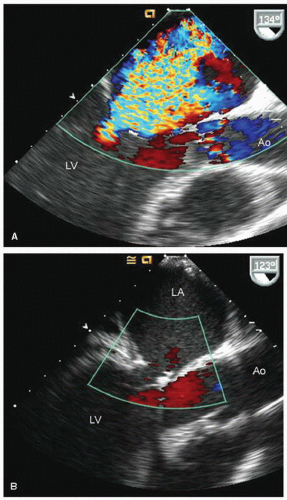 FIGURE 22.31. Color Doppler flow images corresponding to the images presented in Figure 22.30 are shown. A: Note the severe mitral regurgitation arising centrally with the vena contracta location identified by the area of noncoaptation in Figure 22.30. B: A systolic frame recorded after placement of a mitral ring. Note the absence of mitral regurgitation after ring placement. |
valve tissue, this may result in the valve being converted to a nearly unicuspid valve with the anterior leaflet providing the majority of functional valve tissue. More complex repairs may include transposition of a portion of a leaflet and its attached chordae to the opposite leaflet to provide intact chordae to the previously flail leaflet. Finally, prosthetic chords can be attached to a flail mitral leaflet and subsequently to a papillary muscle to replace chordal structures that are damaged beyond repair. The goal of mitral valve repair is to reduce the severity of mitral regurgitation to no more than mild without creating iatrogenic mitral stenosis. In the examples presented, note the smaller annular dimensions due to an annular ring as well as the areas of thickening on the mitral valve that represent areas of resection (Figs. 22.36 and 22.37).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


