History of Echocardiography
Harvey Feigenbaum, M.D.
Many histories of diagnostic ultrasound, and cardiac ultrasound in particular, have been written.1, 2, 3, 4, 5 and 6 They all seem to address this field from a different perspective. One can begin the history in the 20th century, Roman times, or any of the centuries in between. It is stated that a Roman architect, Vitruvius, first coined the word echo.7 A Franciscan friar, Marin Mersenne (1588-1648), is frequently called the “father of acoustics” because he first measured the velocity of sound.7 Another early physicist, Robert Boyle (1627-1691), recognized that a medium was necessary for the propagation of sound.7 Abbe Lazzaro Spallanzani (1727-1799) is frequently referred to as the “father of ultrasound.”8 He demonstrated that bats were blind and in fact navigated by means of echo reflection using inaudible sound. In 1842, Christian Johann Doppler (1803-1853) noted that the pitch of a sound wave varied if the source of the sound was moving.9 He worked out the mathematical relationship between the pitch and the relative motion of the source and the observer. The ability to create ultrasonic waves came in 1880 with the discovery of piezoelectricity by Curie and Curie.10,11 They noted that if certain crystalline materials are compressed, an electric charge is produced between the opposite surfaces. They then noted that the reverse was also true. If an electrical potential is applied to a crystal, it is compressed and decompressed depending on the polarity of the electric charge, and thus very high frequency sound can be produced. In 1912, a British engineer, L. F. Richardson, suggested that an echo technique could be used to detect underwater objects. Later during World War I, Paul Langevin was given the duty of detecting enemy submarines using sound, which culminated in the development of sonar.3 Sokolov12 described a method for using reflected sound to detect metal flaws in 1929. In 1942, Floyd Firestone,13 an American engineer, began to apply this technique and received a patent. It is this flaw detection technique that ultimately was used in medicine.
An Austrian, Karl Dussik,14 was probably the first to apply ultrasound for medical diagnosis in 1941. He initially attempted to outline the ventricles of the brain. His approach used transmission ultrasound rather than reflected ultrasound. After World War II, many of the technologies developed during that war, including sonar, were applied for peaceful and medical uses. In 1950, W. D. Keidel,15 a German investigator, used ultrasound to examine the heart. His technique was to transmit ultrasonic waves through the heart and record the effect of ultrasound on the other side of the chest. The purpose of his work was to try to determine cardiac volumes. The first effort to use pulse-reflected ultrasound, as described by Firestone, to examine the heart was initiated by Dr. Helmut Hertz of Sweden. He was familiar with Firestone’s observations and in 1953 obtained a commercial ultrasonoscope, which was being used for nondestructive testing. He then collaborated with Dr. Inge Edler, who was a practicing cardiologist in Lund, Sweden. The two of them began to use this commercial ultrasonoscope to examine the heart. This collaboration is commonly accepted as the beginning of clinical echocardiography as we know it today.16
The original instrument (Fig. 1.1) was quite insensitive. The only cardiac structures that they could record initially were from the back wall of the heart. In retrospect, these echoes probably came from the posterior left ventricular wall. With some modification of their instrument, they were able to record an echo from the anterior leaflet of the mitral valve. However, they did not recognize the source of this echo for several years and originally attributed the signal to the anterior left atrial wall. Only after some autopsy investigations did they recognize the echo’s true origin. Edler17 went on to perform a number of ultrasonic studies of the heart. Many of the cardiac echoes currently used were first described by him. However, the principal clinical application of echocardiography developed by Edler18 was the detection of mitral stenosis. He noted that there was a difference between the pattern of motion of the anterior mitral leaflet in patients who did or did not have mitral stenosis. Thus, the early studies published in the mid-1950s and early 1960s primarily dealt with the detection of this disorder.
The work being done in Sweden was duplicated by a group in Germany headed by Dr. Sven Effert.19,20 Their publications began to appear in the late 1950s and were primarily duplications of Edler’s work describing mitral stenosis. One notable observation made by Effert and his group20 was the detection of left atrial masses. Schmitt and Braun21 in Germany also began working with ultrasound cardiography and published their work in 1958, again repeating what Edler and Effert had been doing. Edler and his coworkers22 developed a scientific film that was shown at the Third European Congress of Cardiology in Rome in 1960. Edler et al.23 also wrote a large review of cardiac ultrasound as a supplement to Acta Medica Scandinavica, which was published in 1961, and remained the most comprehensive review of this field for more than 10 years. In the movie
and the review, Edler and his coinvestigators described the ultrasonic techniques for the detection of mitral stenosis, left atrial tumors, aortic stenosis, and anterior pericardial effusion.
and the review, Edler and his coinvestigators described the ultrasonic techniques for the detection of mitral stenosis, left atrial tumors, aortic stenosis, and anterior pericardial effusion.
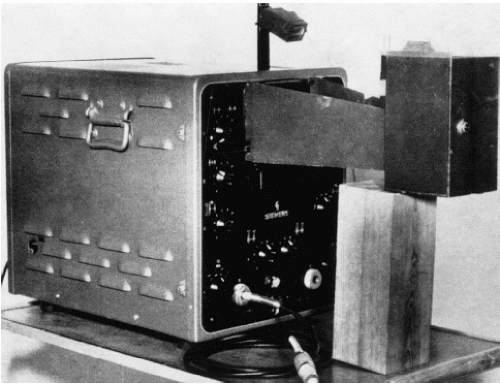 FIGURE 1.1. Ultrasonoscope initially used by Edler and Hertz for recording their early echocardiograms. (From Edler I, Ultrasound cardiography. Acta Med Scand Suppl 370 1961; 170:39.) |
Despite their initial efforts at using ultrasound to examine the heart, neither Edler nor Hertz really anticipated that this technique would flourish. Helmut Hertz was primarily interested in being able to record the ultrasonic signals. In the process, he developed ink-jet technology and spent only a few years in the field of cardiac ultrasound. He devoted most of the rest of his career to ink-jet technology, for which he held many important patents. He also advised Siemens Corporation, which provided its first ultrasonic instrument, that it should not enter the field of cardiac ultrasound because he personally did not feel that there was a great future in this area (Effert, personal communication, 1996). Edler too did not develop any further techniques in cardiac ultrasound. He retired in 1976 and until then was primarily concerned with the application of echocardiography for mitral stenosis and, to a lesser extent, mitral regurgitation. He never became involved with any of the newer techniques for pericardial effusion or ventricular function.
China was another country where cardiac ultrasound was used in the early years. In the early 1960s, investigators both in Shanghai and Wuhan were using ultrasonic devices to examine the heart. They began initially with an A-mode ultrasound device and then developed an M-mode recorder.24,25 The investigators duplicated the findings of Edler and Effert with regard to mitral stenosis.26 Unique contributions of the Chinese investigators included fetal echocardiography27 and contrast echocardiography, using hydrogen peroxide and then carbon dioxide.28
In the United States, echocardiography was introduced by John J. Wild, H. D. Crawford, and John Reid,29 who examined the excised heart. They were able to identify a myocardial infarction and published their findings in 1957 in the American Heart Journal. Neither Wild nor Reid was a physician. Reid was an engineer who subsequently went to the University of Pennsylvania for his doctorate degree. While there, he wanted to continue his interest in examining the heart ultrasonically. He joined forces with Claude Joyner, who was a practicing cardiologist in Philadelphia. Reid proceeded to build an ultrasonoscope, and Joyner and he began duplicating the work on mitral stenosis that was described by Edler and Effert. This work was published in Circulation in 1963 and represents the first American clinical effort, using pulsed reflected ultrasound to examine the heart.30
I became interested in echocardiography in the latter part of 1963. While operating a hemodynamic laboratory and becoming frustrated with the limitations of cardiac catheterization and angiography, I saw an advertisement from a now defunct company that was claiming that it had an instrument that could measure cardiac volumes with ultrasound. This claim ultimately proved to have no basis. However, when I first saw the ultrasound instrument displayed at the American Heart Association meeting in Los Angeles in 1963, I placed the transducer on my chest and saw a moving echo, which had to be coming from the posterior wall of my heart. This signal undoubtedly was the same echo that Hertz and Edler had noted approximately 10 years earlier. I had the people from the company explain the principles by which such a signal might be generated. I asked them whether fluid in back of the heart would give a different type of a signal, and they said that fluid would be echo free. When I returned to Indiana, I found that the neurologists had an ultrasonoscope that they used for detecting the midline of the brain. Fortunately for me, the instrument was rarely being used and I was able to borrow it. I proceeded to examine more individuals, and again I was able to record an echo from the back wall of the left ventricle. I looked for a patient with pericardial effusion. As predicted, there were now two echoes separated by an echo-free space. The more posterior echo no longer moved, whereas the more anterior echo moved with cardiac motion. We went to the animal laboratory to confirm these findings and thus began my personal career in cardiac ultrasound. This initial paper on pericardial effusion was published in JAMA in 1965.31
Although this phase of the history of echocardiography is commonly considered the origins of the early practice of echocardiography, it should be mentioned that Japanese investigators were working simultaneously using ultrasound to examine the heart. In the mid-1950s, several Japanese investigators such as Satomura, Yoshida, and Nimura at Osaka University were using Doppler technology to examine the heart. They began publishing their work in the mid-1950s.32,33 These efforts laid the basis for much of what we do today with Doppler ultrasound.
The field of cardiac ultrasound has evolved with the efforts of numerous individuals over the past 50 years. This development is an outstanding example of collaboration among physicists, engineers, and clinicians. Each of the cardiac ultrasonic techniques has its own individual history. Even the name echocardiography has a story of its own. Edler and Hertz first called this technique ultrasound cardiography with the abbreviation being UCG. Ultrasound cardiography was a somewhat cumbersome name. The most common use of medical diagnostic ultrasound in the late 1950s and early 1960s was an A-mode technique to detect the midline of the brain. This midline echo would shift if there were an intracranial mass. The technique was known as echoencephalography, and the instrument was an echoencephalograph. It was such an instrument that I borrowed from the neurologists. If the ultrasonic examination of the brain is echoencephalography, then an examination of the heart should be echocardiography. Unfortunately, the abbreviation for an echocardiogram would be ECG, which was already preempted by electrocardiography. We could not use the abbreviation “echo” because it did not differentiate from an echoencephalogram. The reason the term echocardiography finally caught on was because echoencephalography disappeared. No other diagnostic ultrasound technique used the term echo except for the examination of the heart. So, the abbreviation “echo” now stands only for echocardiography and is not confused with any other ultrasonic examination.
Development of Various Echocardiographic Technologies
The story of echocardiography involves the evolution and development of its many modalities such as A-mode, M-mode, contrast, two-dimensional, Doppler, transesophageal, and intravascular applications. The Doppler story is truly lengthy and international. The Japanese began working with Doppler ultrasound in the mid-1950s.32,33 American workers, such as Robert Rushmer in Seattle, were early investigators using Doppler techniques.34 Dr. Rushmer was a recognized expert in cardiac physiology. John Reid later moved to Seattle and joined Rushmer and his group in developing Doppler technology. One of the engineers, Donald Baker, was in that group and developed one of the first pulsed Doppler instruments.35 Eugene Strandness was a vascular surgeon in Seattle using Doppler for peripheral arterial disease.36 European investigators were also very active in using Doppler technology. Several early French workers, namely, Peronneau37 and later Kalmanson,38 wrote extensively on the use of Doppler ultrasound to examine the cardiovascular system. A major development in Doppler ultrasound came when Holen39 and then Hatle40 demonstrated that one could derive hemodynamic information from Doppler ultrasound. They noted that one could use a modified version of the Bernoulli
equation to detect gradients across stenotic valves. The report that the pressure gradient of aortic stenosis could be determined with Doppler ultrasound was probably the development that established Doppler echocardiography as a clinically important technique.
equation to detect gradients across stenotic valves. The report that the pressure gradient of aortic stenosis could be determined with Doppler ultrasound was probably the development that established Doppler echocardiography as a clinically important technique.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


