Fig. 21.1
Possible routes of introduction of the transcatheter aortic valve through the transcervical approach
21.1.2 Access to the Innominate and Right Subclavian Arteries
Injuries of the innominate artery and, especially, the right subclavian artery are difficult to manage due to the location of these vessels and to control of bleeding, which might be very severe [5–9].
These injuries are managed with endovascular stent grafting which is not always possible or with surgical approach, which is technically challenging and associated with significant morbidity and mortality. The traditional surgical way to obtain proximal control requires a median sternotomy for the innominate and proximal right subclavian arteries with potential clavicular resection. Such extensive incisions require lengthy healing and rehabilitation and carry significant morbidities. The combination of the transcervical approach with elevation of the sternum and infraclavicular approach provides the possibility to achieve proximal and distal control of bleeding with application of vascular clamps. After proximal and distal clamping of the subclavian artery, an injury of the subclavian artery can be located and repaired without excessive hurry (Fig. 21.2). This technique was used by us in one patient whose right subclavian artery was injured during insertion of a catheter for dialysis, causing severe intrathoracic haemorrhage, and proved to be easy and highly effective. In this patient, transcervical and infraclavicular approaches were combined with right VATS for removal of blood clots and for additional control of bleeding intraoperatively.
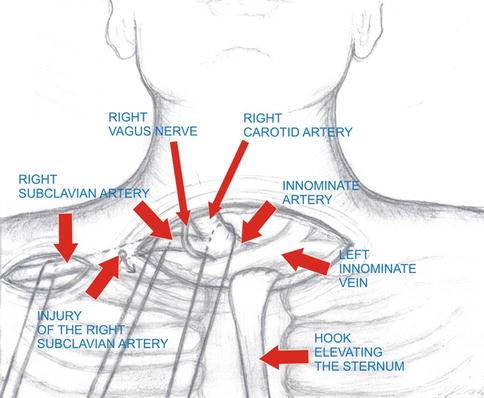
Fig. 21.2
Technique of control of bleeding from the injured right subclavian artery through the transcervical and subclavicular incisions
21.1.3 Expanding Indications for Pulmonary Resections
With the use of the novel retractor for access to the aortopulmonary window, it becomes possible to perform right and left pulmonary lobectomies and, maybe, the other lobectomies with an ease and safety similar to the classic VATS approach. The access provided by the retractors creates a sort of thoracotomy which is bigger that the utility incision used for VATS. Dissection of the vascular structures is done with instruments used for the typical open surgery.
21.1.4 Total Transcervical Oesophagectomy
Most part or even the whole intrathoracic oesophagus, along with the cervical part of the oesophagus with the surrounding lymph nodes, can be dissected under direct eye control through the cervical incision with elevation of the sternum, even with the use of currently available instruments (Fig. 21.3) [10]. Probably, it would be also possible to perform the intra-abdominal part of oesophagectomy. The limit of dissection is the lack of a mediastinoscope of proper length that could reach below the hiatus. Such mediastinoscope should have a curved shape, a sealing system to enable its use while a pneumoperitoneum is created (Fig. 21.4). A camera placed near the tip of such mediastinoscope should enable visualization of the intra-abdominal structures under the proper angle. The next prerequisite would be a special set of instruments long enough to reach the abdominal cavity through the neck incision and adjusted to the curvature of the novel mediastinoscope.
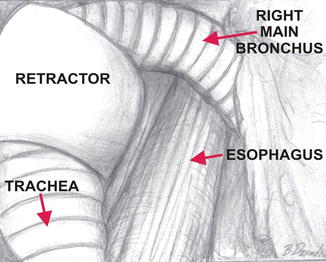
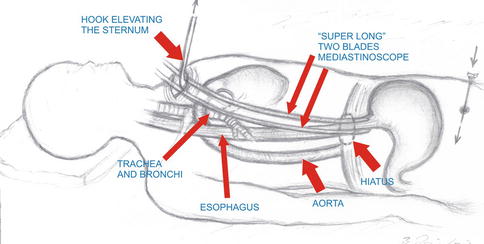
Fig. 21.3
Dissection of the oesophagus through the transcervical incision with elevation of the right main bronchus with use of retractor
Fig. 21.4
Possible technique of oesophagectomy through the sole transcervical incision
Dissection of the whole stomach can be safely performed through the hiatus as was shown by Hiebert and Belsey, who performed the whole oesophagectomy with oesophagogastric anastomosis solely through the right thoracotomy approach [11]. The authors started the dissection blindly from dividing the gastrophrenic and subsequently gastrosplenic ligaments step-by-step by pulling gradually the stomach into the right pleural cavity. It was possible to visualize the left gastric vessels located just caudal to the hiatus and to ligate the vessels separately under direct eye control. A similar sequence of events is possible with the use of the sole transcervical approach with pneumoperitoneum. The whole gastric conduit would be dissected, the lesser curvature would be divided and the specimen (the oesophagus with the lesser curvature) would be extracted through the neck. Afterwards, the gastric conduit would be pulled up to the neck and anastomosed to the remnant of the oesophagus through the cervical incision. Obviously, such an operation could be combined with laparoscopy in case of any intraoperative difficulties.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


