Table 6.1 Linear Measurements of Left Ventricular Size and Function | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
severity of dysfunction if only a normal region is interrogated or overestimate the abnormality if the M-mode beam exclusively transits the wall motion abnormality. A significant limitation of an M-mode measurement of the left ventricle is that it often does not reflect the true minor-axis dimension. This phenomenon is illustrated in Figure 6.2 and is very common in elderly patients in whom there is angulation of the ventricular septum. In this instance, an M-mode beam traverses the ventricle in a tangential manner and overestimates the true internal dimension. As a two-dimensionally guided M-mode cursor must still adhere to beam direction from the transducer, it is often not possible to align the beam truly perpendicular to the long axis of the ventricle so that it reflects the true minor-axis dimension. Newer generation platforms may allow an “anatomical M-mode” beam to be derived from a twodimensional data set and thereby remove this limitation. This may provide a slight advantage for timing events but confers no real advantage over direct two-dimensional measurements for chamber dimensions. When comparisons are made between M-mode and two-dimensional minor-axis dimensions, the M-mode dimension typically overestimates the true minor-axis of the left ventricle by 6 to 12 mm. This systematic discrepancy becomes greater with age and the attendant angulation of the heart. For any given patient, one can generally assume that the degree of off-axis interrogation will remain stable over time and this overestimation will remain constant. As such, in the absence of new regional abnormalities, differences in serial measurements retain their clinical validity, although the actual dimension may be incorrect.
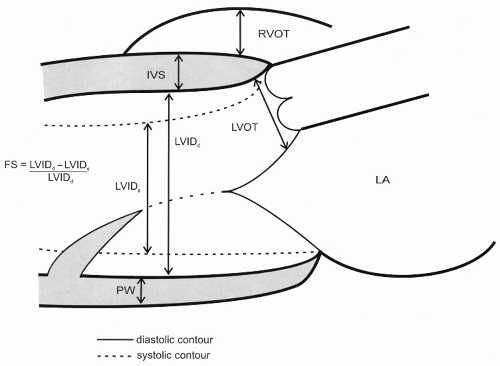 FIGURE 6.1. Schematic of a parasternal long-axis view of the left ventricle depicting linear measurements. By convention, linear measurements of the left ventricle are made at the level of the mitral chordae. From the linear internal dimension of the left ventricle in diastole and systole, fractional shortening can be calculated as noted. When measuring ventricular septal thickness, caution is advised to avoid measuring the most proximal portion of septum, which is frequently an area of isolated hypertrophy and angulation that does not truly represent ventricular wall thickness. FS, fractional shortening; IVS, interventricular septum; LVIDd, left ventricular internal dimension in diastole; LVIDs, left ventricular internal dimension in systole; PW, posterior wall. |
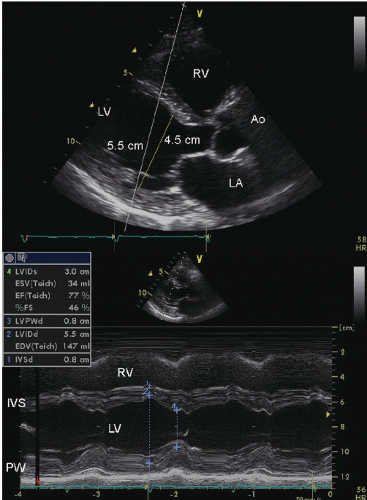 FIGURE 6.2. Parasternal long-axis echocardiogram and two-dimensional-derived M-mode echocardiogram in a patient with normal ventricular function. On the M-mode echocardiogram, note the internal dimension of the left ventricle of 5.5 cm and the derived values. On the two-dimensional echocardiogram, the longer white line represents the M-mode interrogation beam. Note that it traverses the left ventricle in a tangential manner and results in an internal dimension of 5.5 cm. The yellow line is the true short-axis dimension of the left ventricle which is substantially smaller at 4.5 cm. IVS, interventricular septum; PW, posterior wall. |
contraction, the base (annulus) of the heart moves toward the apex. In the presence of global left ventricular dysfunction, the magnitude of this motion is directly proportional to systolic function. M-mode interrogation is undertaken of the lateral mitral annulus, and annular excursion toward the transducer is then calculated (Fig. 6.3). There is a relatively linear correlation between the magnitude of systolic annular excursion and global systolic function. This technique is rarely used today, having given way to direct measures of ventricular volume and ejection fraction. Of note, this same principle is used in Doppler tissue imaging of the annulus for determination of systolic excursion as a marker of ventricular function.
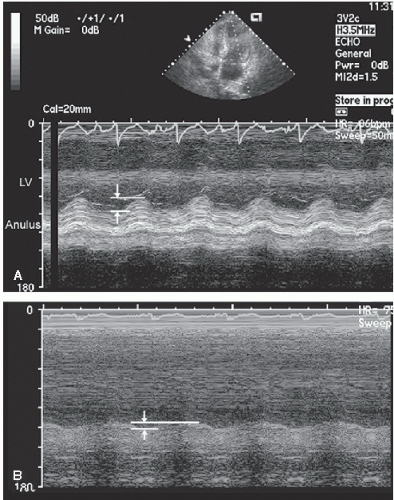 FIGURE 6.3. Apical view recorded in two patients demonstrates the measurement of the descent of the base with M-mode echocardiography. The M-mode interrogation beam has been directed from the apex of the heart through the lateral annulus. A: Note the approximate 1.6 cm of annular motion toward the apex in systole. B: Recording in a patient with severe systolic dysfunction reveals substantially decreased annular motion of <1.0 cm in systole. |
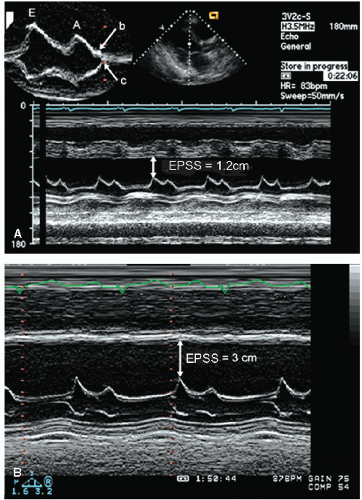 FIGURE 6.4. M-mode echocardiograms recorded in two patients with significant systolic dysfunction. A: An E-point septal separation (EPSS) of 1.2 cm (normal, <6 mm). B: Recording in a patient with more significant left ventricular systolic dysfunction in which the EPSS is 3.0 cm. Also note the interrupted closure of the mitral valve with a B bump (top), indicating an increase in the left ventricular end-diastolic pressure. |
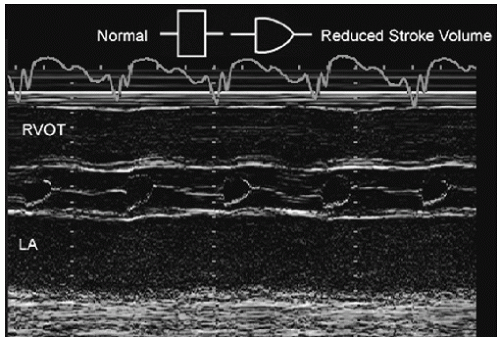 FIGURE 6.5. M-mode echocardiogram recorded through the aortic valve in a patient with reduced cardiac function and decreased forward stroke volume. Note the rounded closure of the aortic valve, indicating decreasing forward flow at the end of systole. Normal and abnormal aortic valve opening patterns are noted in the schematic superimposed on the figure. |
Table 6.2 Area-/Volume-Based Measurements for Ventricular Size and Functiona | ||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||
Table 6.3 Reference Limits and Partition Values of Left Ventricular Sizea | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
“rule of disks.” This technique requires recording an apical, four- and/or two-chamber view from which the endocardial border is outlined in end-diastole and end-systole. The ventricle is mathematically divided along its long axis into a series of disks of equal height. Individual disk volume is calculated as the product of height and disk area, where disc height is assumed to be the total length of the left ventricular long axis ÷ the number of segments or disks. The surface area of each disk is determined from the diameter of the ventricle at that point (area = πr2). The ventricular volume is calculated as the sum of the volume of the disks. This methodology is illustrated in Figure 6.6.
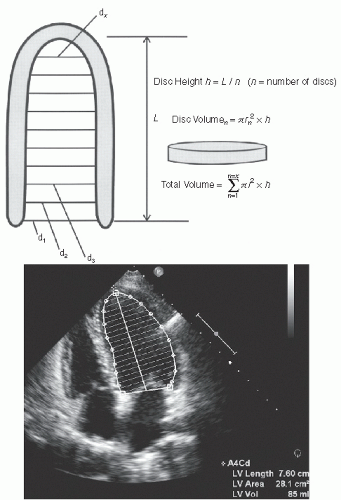 FIGURE 6.6. Schematic illustration of Simpson’s rule or the rule of disks for calculating left ventricular volume. In the upper panel, a schematized left ventricular volume has been subdivided into 10 sections, each of which is presumed to represent a disk of equal diameter at its top and bottom margins. The volume of each disk is calculated as area × height where height is defined as the left ventricular length from apex to base ÷ by the number of disks. The total volume of the ventricle is calculated as the sum of each disk volume. The lower panel is an apical four-chamber view recorded in a normal individual in which this algorithm has been used to calculate a left ventricular volume. |
for the reasons previously alluded to. In this instance, averaging of volumes from multiple views or use of three-dimensional echocardiography will increase accuracy (Fig. 6.8).
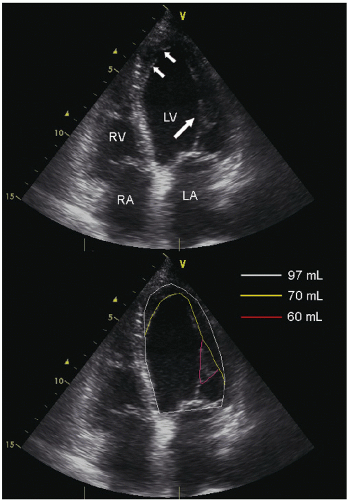 FIGURE 6.7. Apical four-chamber view recorded in a patient with normal ventricular size and function. The upper panel is the apical four-chamber view from which volume can be calculated. Notice the vague echoes at the apical septal and apical lateral wall due to a combination of beam width imaging and trabeculae (arrows) as well as the papillary muscle protruding into the left ventricular cavity (arrow). The lower panel outlines three separate contours which could be drawn from this view. The white line represents the true inner endocardial border of the left ventricle, excluding trabeculation, beam width imaging and the papillary muscle from the cavity, and results in a left ventricle cavity volume of 97 mL. The yellow line excludes the papillary muscle tip but includes the apical trabeculations and tangential beam-related echoes and results in a left ventricular volume of 70 mL. The red line further excludes the papillary muscle tip from the left ventricular volume and would result in a left ventricular volume of 60 mL. |
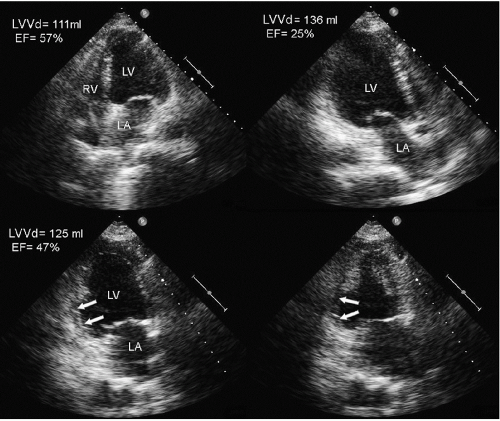 FIGURE 6.8. Apical views recorded in a patient with an extensive inferior-posterior myocardial infarction and basilar inferior aneurysm (arrows). The apical four-chamber view and apical long-axis view are presented in the top panels. The bottom panels are the apical two-chamber view in diastole on the left and systole on the right. The end-diastolic volume and ejection fraction for each view are as noted. Note that if only the four-chamber view is used for analysis, there is a substantial overestimation of ejection fraction as the regional wall motion abnormality is seen only in the two-chamber and apical long-axis views. EF, Ejection fraction; LVVd, left ventricular volume in diastole. |
volume from two-dimensional echocardiography, manual adjustment of the automatically defined ventricular border is commonly necessary. Once generated, the three-dimensional volume can be further subdivided into a 16- or 17-segment model as done with two-dimensional echocardiography. A variety of sophisticated measures of global and regional ventricular function can be extracted from the same three-dimensional volume (Fig. 6.11). The data that can be extracted is platform specific but includes regional volume change in 16- or 17-segments as well as parameters of volume change over time which have shown promise for evaluation of mechanical dyssynchrony. Numerous studies have demonstrated the superiority of threedimensional echocardiography over two-dimensional echocardiography for determination of left ventricular volumes when compared to a standard such as cardiac magnetic resonance imaging (Table 6.4). While the accuracy and inter- and intraobserver reproducibility of left ventricular volumes derived from three-dimensional data sets exceed that of two-dimensional imaging, the magnitude of improvement in accuracy is not always at a level likely to result in a change in clinical decision
making. Most studies have suggested that left ventricular volumes determined with real-time three-dimensional echocardiography underestimate both end-diastolic and end-systolic volume. As with two-dimensional imaging, this is apparently due to inclusion of left ventricular trabeculae and papillary muscles within the cavity and is a more prominent problem with less experienced operators.
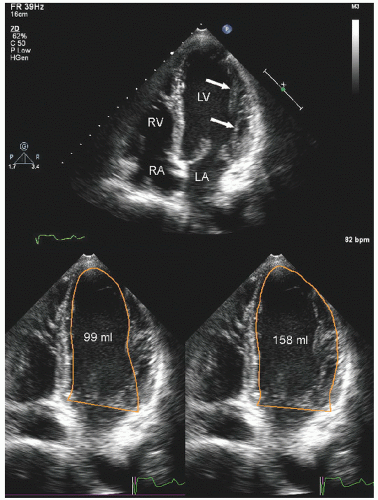 FIGURE 6.9. Apical four-chamber view recorded in a young patient with normal ventricular function and fairly prominent trabeculae along the lateral ventricular wall. The upper panel is an apical four-chamber view in which the papillary muscle and trabeculae can be seen on the lateral wall (arrows). The lower left panel is the initial, unaltered, automatically determined endocardial border from a commercially available platform. Note that the algorithm for identifying the endocardial border has included papillary muscles and the trabeculae within the ventricular cavity which results in a calculated left ventricular volume of 99 mL. The lower right panel was recorded after manual adjustment of the previously automatically determined border. Only the lateral border has required adjustment. After adjustment, notice the calculated left ventricular volume is 158 mL. |
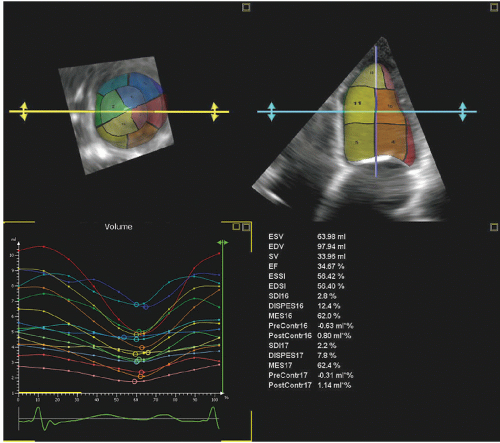 FIGURE 6.10. Reconstructed three-dimensional echocardiogram from a real-time three-dimensional volumetric scanner recorded in a patient with a dilated cardiomyopathy and reduced left ventricular function. The upper two panels depict apical four-chamber and short-axis views extracted from the same three-dimensional data set as well as the corresponding three-dimensional shell subdivided into 17 segments. The lower right table provides automatically extracted measurements including calculation of an ejection fraction of approximately 35%. Parameters of dispersion of contractility based on subvolume analysis, as would be relevant for determination of dyssynchrony, are also provided. The lower left panel is a graph of instantaneous volume change in each of the predefined segments. |
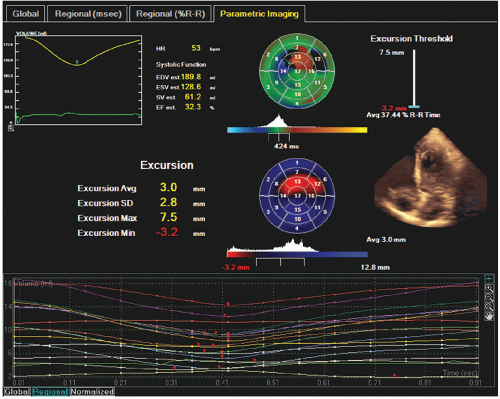 FIGURE 6.11. This illustration depicts multiple parameters of left ventricular function which can be extracted from a single threedimensional volume (small inset). The lower graph is an individual volume curve for 17 subvolumes in a patient with a dilated cardiomyopathy and an ejection fraction of approximately 32%. From this volume, end-diastolic and end-systolic volumes (EDV, ESV) as well as stroke volumes (SV) and ejection fraction are all calculated. In addition, polar maps are derived from endocardial excursion in each of 17 segments and expressed as an average, standard deviation, maximum and minimum excursion. The timing to maximum excursion is also depicted as a histogram. Various parameters are available for determination of global and regional left ventricular function as well as for timing of contraction which may have relevance for decision making regarding resynchronization therapy, all of which are extracted from a single three-dimensional volume. |
Table 6.4 Accuracy of Three-dimensional Echocardiography for Determination of Left Ventricular Volumea | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
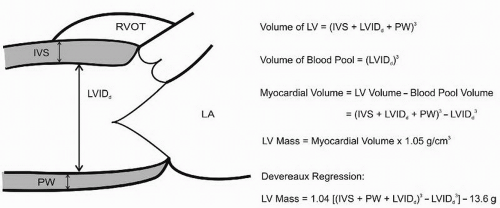 FIGURE 6.12. Schematic representation of the cubed formula for determining left ventricular mass. All measurements can be taken from either a two-dimensional or an M-mode echocardiogram of the minor axis of the left ventricle. The formula for calculation of left ventricular mass is as noted. Based on comparison with anatomic specimens, several regression equations have been developed that are variations on the basic cubed formula. IVS, interventricular septum; LVIDd, left ventricular internal dimension in diastole; PW, posterior wall. |
by determining the epicardial and endocardial areas of the short-axis of the left ventricle at the midcavity level. The difference between these two areas then represents myocardial area. Left ventricular mass can then be calculated either by an area length method or by assuming a truncated ellipse geometry. Figure 6.14 depicts this approach and provides formulas used for calculation of left ventricular mass with this technique. More recently, three-dimensional echocardiography has been used to extract epicardial and endocardial borders from multiple orthogonal planes, from which left ventricular mass can be determined in a similar manner. Limited studies have suggested excellent correlation of three-dimensional mass with anatomic and magnetic resonance imaging as standards.
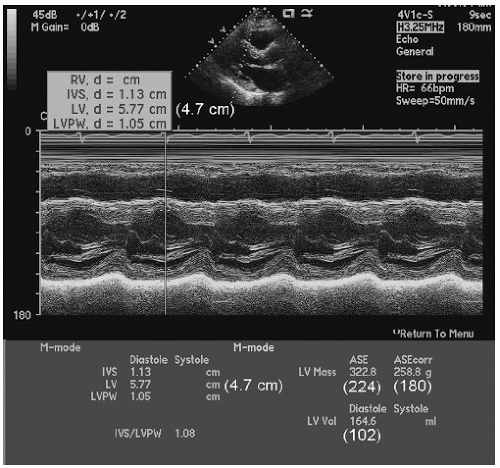 FIGURE 6.13. Two-dimensionally guided M-mode echocardiogram recorded in a patient with mild hypertension. Note in the small inset, the tangential M-mode interrogation beam which is a result of beam orientation and slight angulation of the heart. The M-mode is as displayed from which a left ventricular internal dimension of 5.77 cm is measured. The true minor axis dimension of the left ventricle is 4.7 cm. The bottom panel represents the calculated M-mode report from the measured values. The numbers in parentheses are the corresponding values from a true minor axis dimension (4.7 cm) used rather than the off-axis 5.77 cm. Note the substantial overstatement of left ventricular mass using the dedicated M-mode measurement versus a true minor axis dimension from the two-dimensional echocardiogram. |
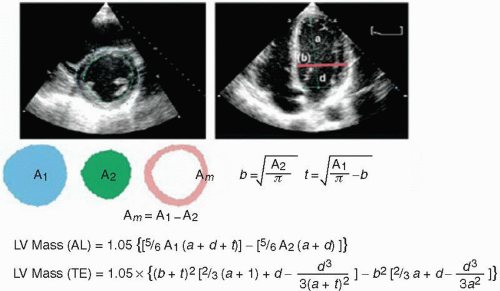 FIGURE 6.14. Demonstration of the methodology for determining left ventricular mass from two-dimensional echocardiography. Mean wall thickness is calculated by tracing the epicardial and endocardial boundaries (A1, A2) and average mass (Am) calculated as the difference between the two. Left ventricular mass can then be calculated using an area length (AL) or a truncated ellipse (TE) formula. (Reproduced with permission from the American Society of Echocardiography from Recommendations for Chamber Quantification: a report from the ASE Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. JASE 2005;18:1440-1463.) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


