Table 24.1 Appropriateness Criteria for the Application of Echocardiography in systemic Disease and Clinical decision Making | ||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 24.2 Systemic diseases and Clinical Presentations in Which Echocardiography Plays a Valuable Role | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
reported in preclinical infiltrative and hypertrophic cardiomyopathies and are likely present in a broad range of othe disease states as well. As such, their utilization clearly needs to be put in context of the clinical situation.
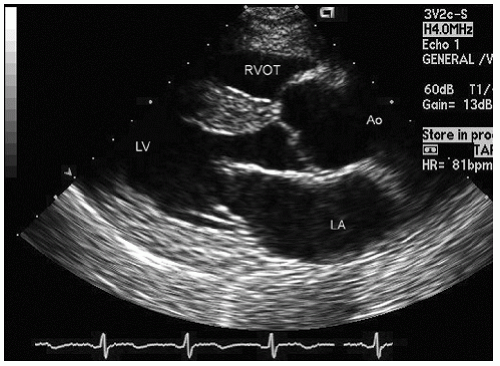 FIGURE 24.1. Parasternal long-axis view recorded in a 30-year-old patient with essential hypertension. In this diastolic frame, note the mild left ventricular hypertrophy but otherwise normal anatomy and preserved systolic function in the real-time image. |
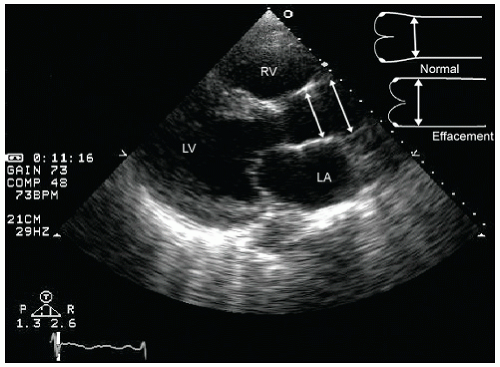 FIGURE 24.2. Parasternal long-axis image recorded in a patient with severe long-standing and poorly controlled hypertension. Note the left ventricular hypertrophy and the mild left atrial dilation. In the real-time image, note the global hypokinesis of the left ventricle. Also note the dilation of the ascending aorta with effacement at the sinotubular junction. |
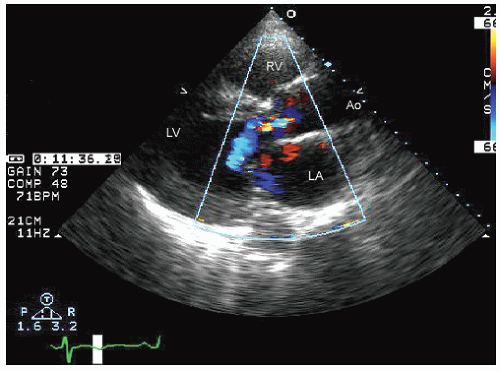 FIGURE 24.3. Parasternal long-axis echocardiogram with color Doppler flow imaging recorded from the same patient presented in Figure 24.2. Note the effacement of the sinotubular junction, which results in malcoaptation of the aortic cusps and a central aortic regurgitation jet. |
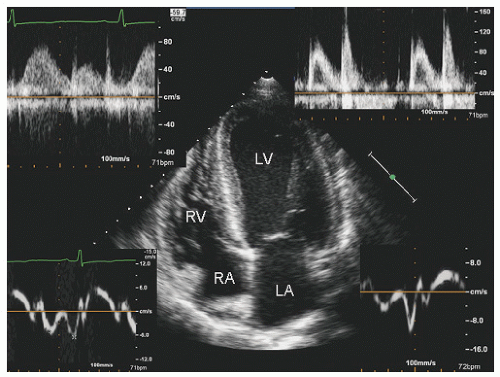 FIGURE 24.4. Apical four-chamber view with mitral inflow, pulmonary vein flow, and Doppler tissue imaging of the annulus in a patient with essential hypertension. Note the reversal of the mitral E/A ratio, which is paralleled by reversal of annular velocities, all consistent with grade 1 diastolic dysfunction in this otherwise healthy 45-year-old patient. reported in preclinical infiltrative and hypertrophic cardiomyopathies and are likely present in a broad range of other disease states as well. As such, their utilization clearly needs to be put in context of the clinical situation. |
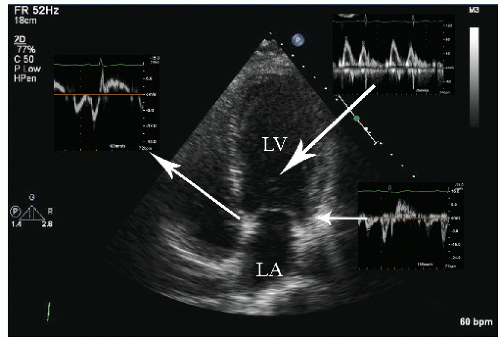 FIGURE 24.5. Apical four-chamber view with multiple Doppler images in a 32-year-old female patient with diabetes but no evidence of hypertension or coronary artery disease. The geometry and size of the left ventricle are normal without evidence of overt left ventricular hypertrophy. Notice the pseudonormal mitral inflow with a mitral E/A ratio of approximately 1.2, but the reversed annular e′/a′ ratio of both the septal and lateral mitral annulus implying diastolic dysfunction. |
 FIGURE 24.6. Doppler tissue based strain imaging recorded from the same patient depicted in Figure 24.5. The strain images reveal reduced mean strain predominantly in the lateral wall with a lesser reduction in the two septal segments. |
include left ventricular hypertrophy due to hypertension and an abnormal texture of the hypertrophied myocardium that mimics that seen in cardiac amyloid (Fig. 24.10). Other abnormalities seen in chronic renal insufficiency include pericardial effusion, which may range from small chronic effusions to presentation with cardiac tamponade. Uremia results in inflammatory and occasionally hemorrhagic pericarditis in which there is often evidence of “stranding” on the visceral pericardium (Figs. 24.11 and 24.12).
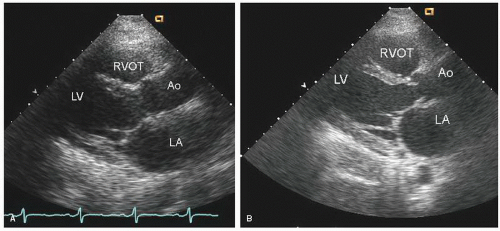 FIGURE 24.7. Parasternal long-axis echocardiograms recorded at end systole in a patient with severe thyrotoxicosis who presented with nonsustained ventricular tachycardia and congestive heart failure. A: Note the relatively preserved left ventricular internal dimension (52 mm) but the severe hypokinesis in systole in the real-time image. B: Recorded 6 months later, after successful therapy, and confirms substantial recovery of systolic function. |
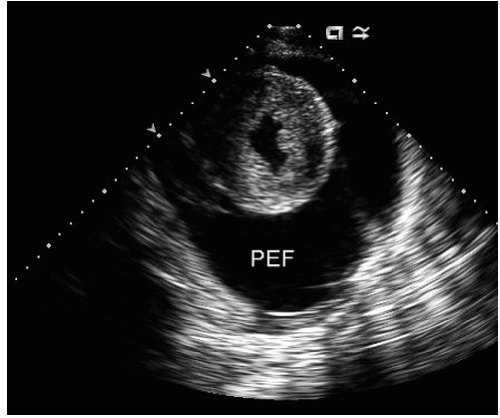 FIGURE 24.8. Echocardiogram recorded in a patient with profound hypothyroidism (TSH > 300). Note the large pericardial effusion (PEF) with a swinging heart in the real-time image. The patient had no clinical evidence of hemodynamic compromise. Incidental note is made of severe left ventricular hypertrophy, presumably related to long-standing hypertension. |
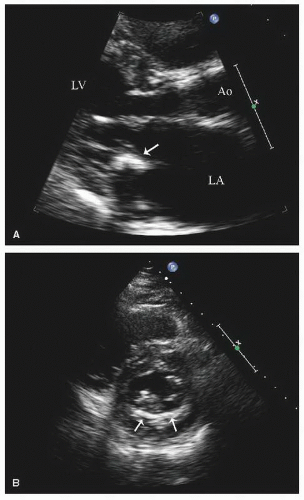 FIGURE 24.9. Parasternal long- and short-axis echocardiograms recorded in a patient with chronic renal insufficiency and calcification of the mitral annulus. A: In the parasternal long-axis view, notice the focal deposits in the posterior annulus (arrow), which have resulted in a side lobe artifact mimicking an associated mass. B: In the short-axis view, notice the crescent of calcium encompassing the posterior mitral annulus (arrows). |
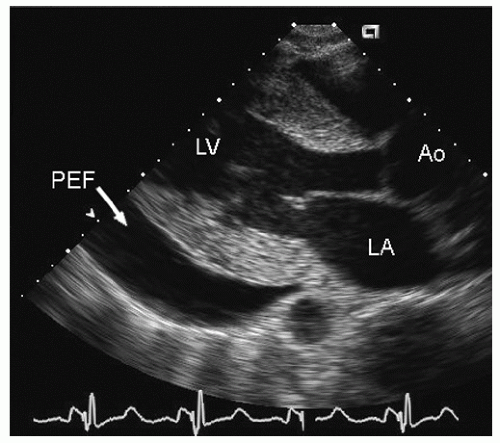 FIGURE 24.10. Parasternal long-axis echocardiogram recorded in a patient with end-stage renal disease. Left ventricular hypertrophy with abnormal myocardial texture, as well as a moderate pericardial effusion (PEF), is present. |
reported in which systolic function recovers after institution of more aggressive dialysis or renal transplantation. Figure 24.13 was recorded in a 34-year-old patient with end-stage renal disease related to glomerulonephritis. Note the significant systolic dysfunction in the real-time images and evidence of marked diastolic dysfunction. Figure 24.14 was recorded 6 months after renal transplantation and demonstrates marked reversal of both the systolic and diastolic dysfunction.
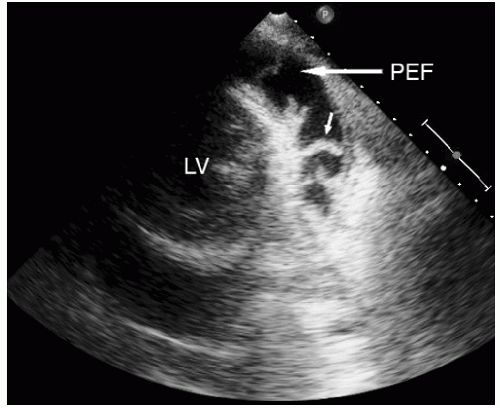 FIGURE 24.11. Parasternal short-axis view recorded in a patient with chronic renal insufficiency and uremic pericarditis. Note the moderate pericardial effusion (PEF) and the multiple strands connecting the visceral and parietal pericardium (arrow). |
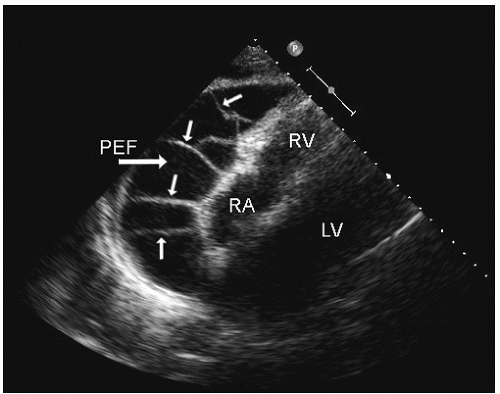 FIGURE 24.12. Subcostal echocardiogram recorded in a patient with chronic renal insufficiency and a large pericardial effusion (PEF) localized over the right atrium (RA) and right ventricle. Again, note the stranding between the visceral and parietal pericardium, implying a marked inflammatory response. |
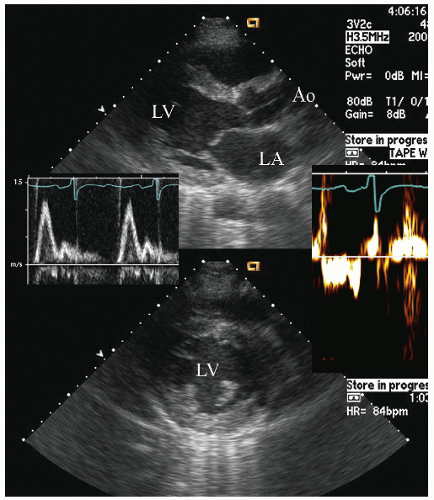 FIGURE 24.13. Parasternal long-and short-axis echocardiogram recorded in a patient with chronic renal insufficiency (known not to have coronary artery disease). In the real-time images, note the global hypokineses of the ventricle and the mildly abnormal myocardial texture. The Doppler insets demonstrate an elevated mitral E/A ratio with reduced annular e’/a’ ratio implying restrictive physiology. |
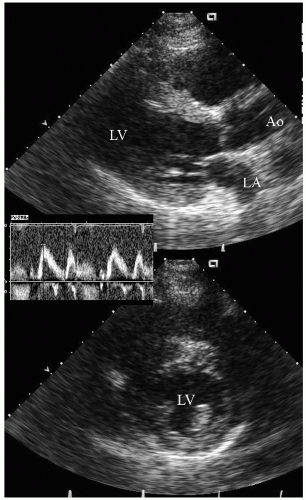 FIGURE 24.14. Parasternal long- and short-axis echocardiogram recorded 6 months after renal transplantation in the same patient depicted in Figure 24.13. In the real-time images, note the almost complete recovery of systolic function. Also note the normalization of mitral inflow. |
are no characteristic features of the pericarditis or pericardial infusion seen in SLE. On rare occasion, SLE has been associated with pulmonary hypertension, although this association is far more common with scleroderma.
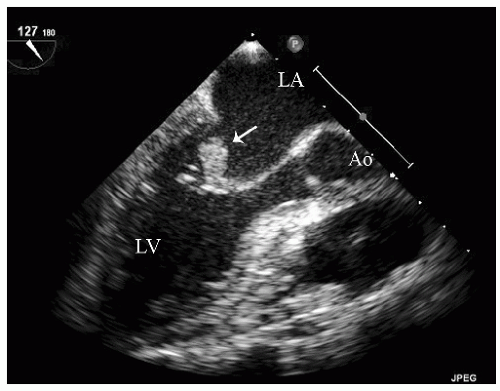 FIGURE 24.15. Transesophageal echocardiogram recorded in a patient with systemic lupus erythematosus and a neurologic event. Note the mobile mass on the atrial aspect of the mitral leaflet (arrow) representing a presumed Libman-Sacks vegetation in this patient without evidence of an infectious process. |
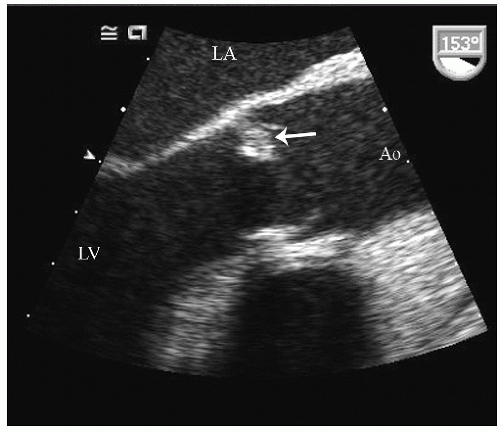 FIGURE 24.16. Transesophageal echocardiogram recorded in a longitudinal view of the aorta revealing a mass on the ventricular aspect of the aortic cusp in a patient with systemic lupus erythematosus, representing a Libman-Sacks vegetation. |
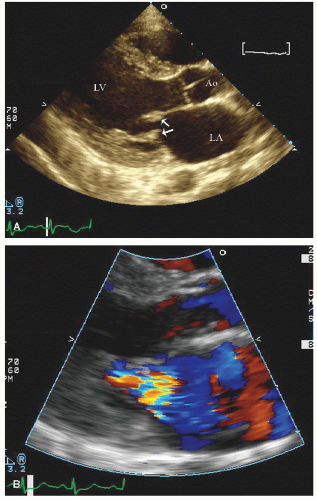 FIGURE 24.17. Parasternal long-axis view in a patient with connective tissue disease and documented antiphospholipid antibody syndrome. Note the small, immobile masses on the atrial aspect of both the anterior and posterior mitral valve leaflets (arrows) (A) and the moderate mitral regurgitation on color flow Doppler imaging (B). |
primary pulmonary hypertension with an increase in pulmonary vascular resistance at the arteriolar level (Fig. 24.19). Concurrent pericardial effusion may be more common in scleroderma than in pulmonary hypertension of other etiologies and is not necessarily an indicator of end-stage disease. The manifestations of pulmonary hypertension as a distinct entity are discussed further in this chapter, and the echocardiographic features of right ventricular pressure overload have been discussed in Chapters 8 and 13.
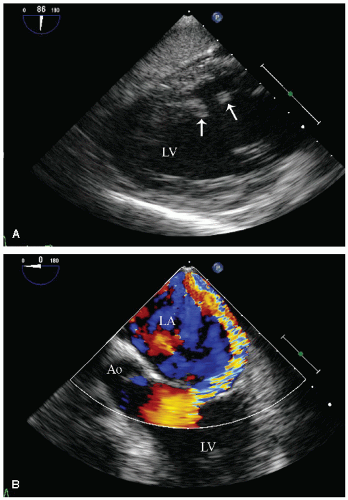 FIGURE 24.18. Transesophageal echocardiogram recorded in a 24-year-old patient with connective tissue disease and evidence of catastrophic antiphospholipid antibody syndrome. Note the rupture of the papillary muscle (arrows) (A) and the highly eccentric mitral regurgitation jet related to a flail mitral leaflet (B). |
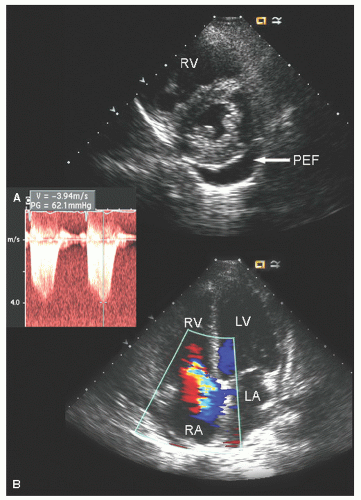 FIGURE 24.19. Transthoracic echocardiogram recorded in a patient with scleroderma and pulmonary hypertension. A: Note the small pericardial effusion (PEF) as well as the dilation of the right ventricle and the right ventricular overload pattern on the ventricular septum. B: In the apical four-chamber view, note the marked right heart dilation with tricuspid regurgitation. In the inset, note the elevated tricuspid regurgitation jet velocity consistent with significant pulmonary hypertension. |
as a cause of aortic insufficiency. Dilation of the actual aortic annulus is uncommon, and in most patients, aortic insufficiency is the result of effacement of the sinotubular junction and not an abnormality of the annulus.
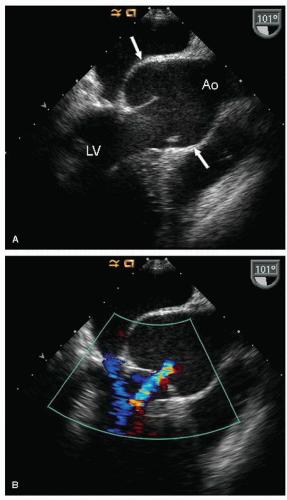 FIGURE 24.20. Transesophageal longitudinal view of the ascending aorta in a patient with Marfan syndrome. A: Note the dilation of the proximal aorta, confined to the sinus of Valsalva with relatively normal dimensions of the sinotubular junction and ascending Ao. B: Color flow Doppler demonstrates mild aortic regurgitation, which is a result of malcoaptation of the aortic cusps. |
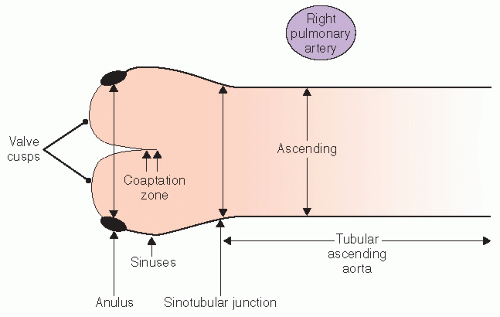 FIGURE 24.21. Schematic representation of normal aortic anatomy and the different components of the proximal aorta as well as recommended sites for making measurements. |
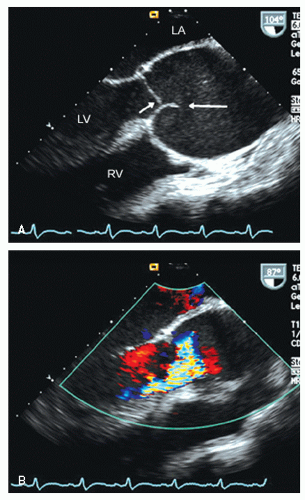 FIGURE 24.22. Transesophageal echocardiogram recorded in a patient with Marfan syndrome and marked proximal aortic dilation. There is significant effacement of the sinotubular junction resulting in malcoaptation of the aortic cusps. Note the relatively normal position in diastole of the right aortic cusp (horizontalarrow (A) and the abnormal closure position of the noncoronary cusp, which fails to contact the opposing cusp, resulting in a highly eccentric aortic regurgitation jet (B). |
a patient should undergo an evaluation of the entire extent of at least the thoracic aorta, which can be performed with transesophageal echocardiography, computed tomography, or magnetic resonance imaging. If there is no evidence of distal aortic dilation, follow-up usually can be performed with transthoracic echocardiography because the proximal ascending aorta is the single most likely site to be involved in subsequent dilation. It should be emphasized that follow-up should include serial measurements as noted previously for comparison. A maximum aortic dimension of 55 mm is considered an indication for elective surgical intervention. However, a threshold of 50 mm has been recommended in the presence of a bicuspid aortic valve or in the Marfan syndrome and is also used as a general indication in high-volume centers. In addition, an interval increase in size of 5 mm over a period of 12 months or less is considered an indication for prophylactic aortic replacement. The need to index aortic size to body size is not firmly established; however, the implications of dilation less than 55 mm in a smallstatured individual are obvious. Aortic dilation associated with clinically relevant aortic insufficiency has been considered an indication for surgery as well. After surgical repair, continued surveillance is crucial because this is a systemic process involving all portions of the aorta. However, after replacement of the ascending aorta in a patient with Marfan syndrome, follow-up may require transesophageal echocardiography, computed tomography, or magnetic resonance imaging because additional disease will typically not be in the field of view of transthoracic echocardiography.
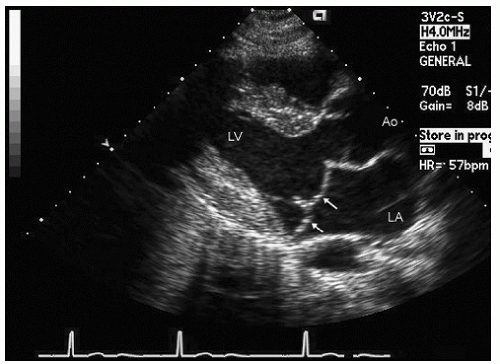 FIGURE 24.23. Parasternal long-axis echocardiogram recorded in a young patient with Marfan syndrome and only mild dilation of the ascending aorta. This patient also has classic mitral valve prolapse (arrows). |
pressures with hepatic congestion result in an obstructive biochemical pattern.
Table 24.3 Heart and Liver Disease | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||
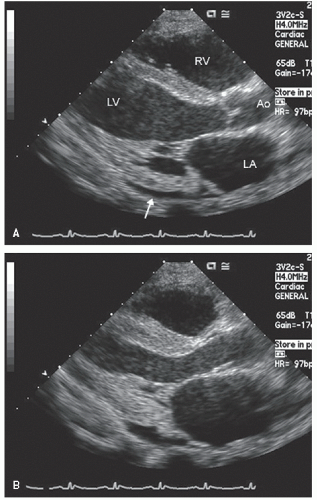 FIGURE 24.24. Parasternal long-axis viewrecorded in diastole(A) and systole (B) in a patient with end-stage liver disease and a high-output state. Resting cardiac output was 16 L/min in the catheterization laboratory. Note the mild dilation of the left atrium and left ventricle and the hyperdynamic motion of the left ventricle at rest. Incidental note is made of a small pericardial effusion (arrow). |
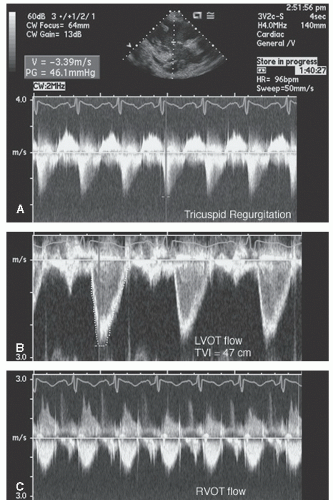 FIGURE 24.25. Spectral Doppler imaging recorded in the patient presented in Figure 24.24. Note the peak tricuspid regurgitation velocity of 3.4 m/sec and the greater than usual time velocity integral (TVI)of both left ventricular outflow tract and right ventricular outflow tract. |
pathologic right-to-left shunt due to pulmonary AVMs. If the magnitude of shunting is significant, percutaneous closure of the pulmonary AVM may be beneficial. Identification of such a shunt also assists in clinical management because it may provide an explanation for otherwise unexplained arterial desaturation.
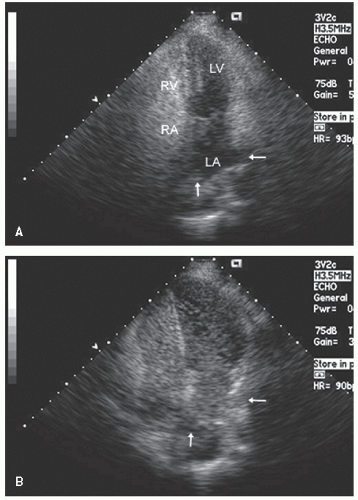 FIGURE 24.26. Apical four-chamber view with intravenous saline contrast recorded in a patient with end-stage liver disease and pulmonary arterial venous malformations. A: Contrast is present in the right atrium and right ventricle but has not yet appeared in the left atrium or left ventricle. The two pulmonary veins are free of contrast (arrows). B: Recorded 27 seconds after image A and shows opacification of the left atrium and left ventricle. Note also that the contrast can be clearly seen in the pulmonary veins (arrows), documenting that the level of shunt is not directly at the atrial level but rather due to a pulmonary arteriovenous malformation. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


