Chapter 10 Drug Effects, Electrolyte Abnormalities, and Metabolic Factors
Drug Effects
Drugs Used to Treat Arrhythmias
Cardiologists often use a shorthand classification system when referring to drugs primarily used to treat arrhythmias (Box 10-1). This system has a number of flaws, but is widely employed—so students and clinicians need to be aware of it.
BOX 10-1 Commonly Used Classification of Drugs Used to Treat Arrhythmias
Class 1: Sodium channel blocking (conduction slowing) effects
Class 2: Beta-blocking effects (examples: atenolol; carvedilol; metoprolol; propranolol)
Class 3: Potassium channel (repolarization) blocking effects (examples: amiodarone; dofetilide; dronedarone; ibutilide; sotalol)
Class 4: Calcium channel blocking effects (examples: diltiazem; verapamil)
Class 5: Other (examples: glycosides, such as digoxin; adenosine)
Class 1 drugs have a sodium channel blocking action, so they may prolong the QRS duration. The class I drugs are subdivided into A, B, and C groups. Class 1A drugs also prolong repolarization via potassium channel blocking effects. Therefore, they may prolong the QT(U) interval, leading to increased risk of torsades de pointes and sudden cardiac arrest (Chapters 16 and 19; Figs. 2-13 and 19-7). Class 1B drugs include lidocaine and mexiletine. Class IC drugs, such as flecainide and propafenone, used to treat atrial fibrillation and other supraventricular tachycardias, are the most likely to produce clinically important widening of the QRS complex (intraventricular conduction delays) due to their prominent sodium channel blocking effects.
All “antiarrhythmic” class 1 (sodium channel blocking) drugs, along with many other pharmaceutical agents, may, paradoxically, induce or promote the occurrence of life-threatening ventricular arrhythmias by altering basic electrical properties of myocardial cells. These so-called proarrhythmic drug effects, which are of major clinical importance, are discussed further in Chapters 16 and 19.
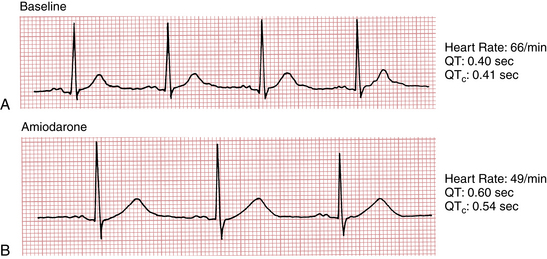
Prolongation of the QT(U) interval with a life-threatening risk of torsades de pointes, another type of ventricular proarrhythmia, can also occur with class 3 drugs, notably ibutilide, dofetilide, sotalol (also has beta-blocking effects), amiodarone (also beta-blocking, among other, effects), and dronedarone (Fig. 10-1). This effect is also related to blocking of potassium channel function with prolongation of myocardial cellular repolarization.
Weaknesses of this classification scheme include its failure to account for drugs with “mixed” effects (like amiodarone and sotalol) and the fact that important drugs, such as adenosine and digoxin, do not fit in. Instead, they are placed under the class 5 or “other” category. The therapeutic and toxic effects of digitalis-related drugs, like digoxin, are discussed separately in Chapter 18.
Psychotropic and Related Drugs
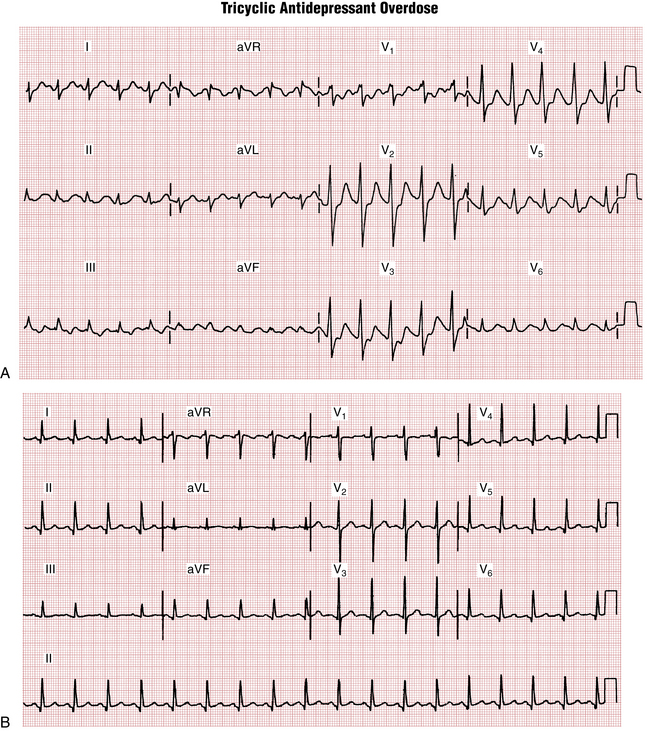
Psychotropic drugs (e.g., phenothiazines and tricyclic antidepressants) can markedly alter the ECG and in toxic doses can induce syncope or cardiac arrest due to a ventricular tachyarrhythmia or asystole. They may also prolong the QRS interval, causing a bundle branch block–like pattern, or they may lengthen repolarization (long QT-U intervals), predisposing patients to develop torsades de pointes. Figure 10-2 presents the classic ECG findings of tricyclic antidepressant overdose, in this case in a young adult. Notice the prolonged QRS and QT intervals, as well as sinus tachycardia.