contributes to the deterioration of systolic function because the spherical geometry interferes with contractile efficiency. Normally, the long axis dimension of the left ventricle exceeds the minor axis dimension (diameter) with a ratio of 1.6:1 or greater. With progressive dilation, the minor axis increases disproportionally, and the ratio of long to minor axis decreases. Typically, a ratio (sphericity index) of less than 1.5:1 implies pathologic remodeling. The increasing spherical geometry results in apical and lateral displacement of the papillary muscles. This effectively reduces the length of the mitral apparatus and results in functional mitral regurgitation.
Table 18.1 Classification of Cardiomyopathy and Diseases Resulting in Acute or Chronic Left Ventricular Dysfunction | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 18.2 Appropriateness Criteria for Echocardiography in Cardiomyopathy and Congestive Heart Failure | ||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||
Figure 18.1. Figure 18.5 depicts secondary mitral regurgitation due to apical and lateral displacement of the papillary muscles, resulting in abnormal coaptation of the mitral valve leaflets.
Table 18.3 Echocardiographic Abnormalities in Cardiomyopathy | |||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||
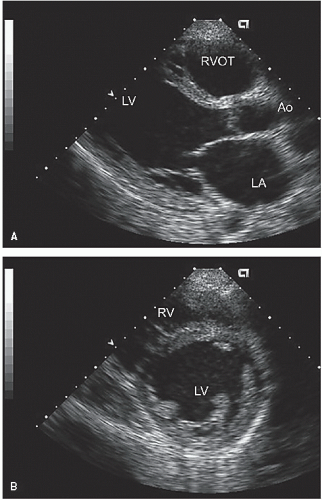 FIGURE 18.1. Parasternal views recorded in a patient with a dilated cardiomyopathy. A: In the parasternal long-axis view, note the dilation of the left ventricle (65 mm) and left atrium (50 mm). B: In the short axis view, note the normal circular geometry of the left ventricle and the uniform wall thickness. In real-time, all walls are uniformly hypokinetic. |
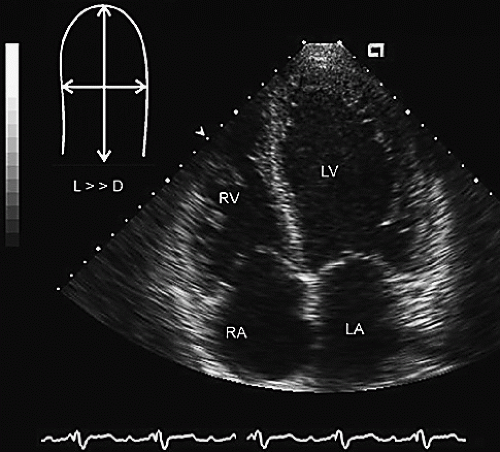 FIGURE 18.2. Apical four-chamber view recorded in the same patient as in Figure 18.1. In this example, normal left ventricular geometry has been preserved, with a long-axis dimension significantly greater than the short-axis dimension, as noted in the schematic in the upper left. |
point (E-point) of the mitral valve (Fig. 18.7). Because the internal dimension of the left ventricle is proportional to diastolic left ventricular volume and the maximal diastolic excursion of the mitral valve is proportional to mitral stroke volume, the ratio of the two dimensions will be proportional to the ejection fraction. As such, limited mitral valve opening (manifested by a greater distance between the E-point and the septum) is an indirect indicator of reduced ejection fraction. The normal EPSS is 6 mm, with progressively larger EPSS representing lower ejection fraction. Evaluation of aortic valve motion also provides clues to left ventricular performance. Normally, the aortic valve has crisp opening and closing points and as such opens as a “box” when imaged with M-mode echocardiography. Reduced forward flow results in a more gradual closure during systole so that there is rounding of the aortic valve closing due to reduced forward flow (Fig. 18.8).
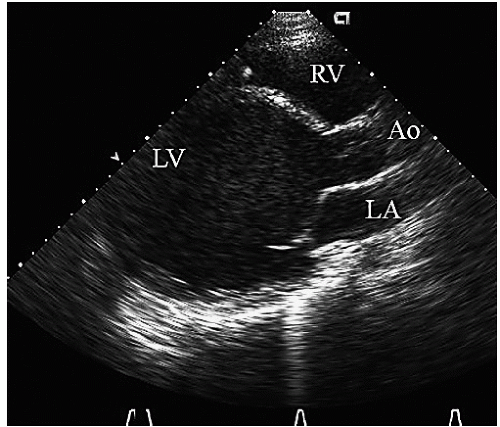 FIGURE 18.3. Parasternal long-axis view recorded in a patient with a long-standing, idiopathic dilated cardiomyopathy revealing marked dilation of the left ventricle but relatively preserved left atrial and right ventricular size. In the real-time image, note the severe global hypokinesis and spherical geometry of the ventricle. |
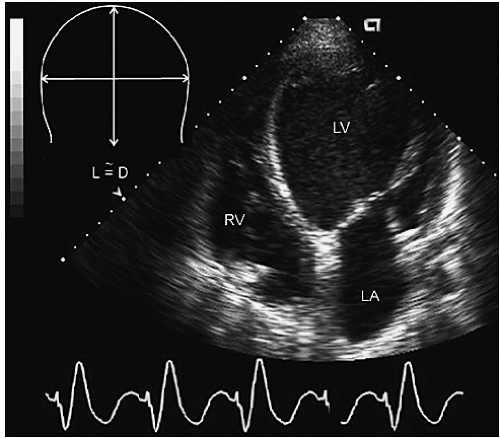 FIGURE 18.4. Apical four-chamber view recorded in a patient with a dilated cardiomyopathy and spherical ventricular geometry in which the long- and short-axis dimensions are essentially equal. This has resulted in lateral displacement of the papillary muscles and retraction of the mitral apparatus toward the apex. |
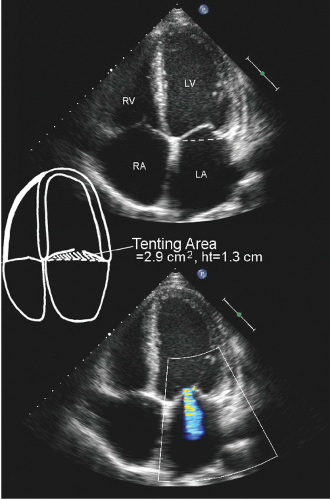 FIGURE 18.5. Apical four-chamber view recorded in a patient with a nonischemic dilated cardiomyopathy. Note the biatrial enlargement as well as the left ventricular enlargement and global hypokinesis. In the color flow image, note the functional mitral regurgitation. In the upper panel, note the coaptation of the mitral valve well above the plane of the annulus (dotted line), which is also schematized. Both the tenting area and height, which are related to severity of functional mitral regurgitation, are as noted. |
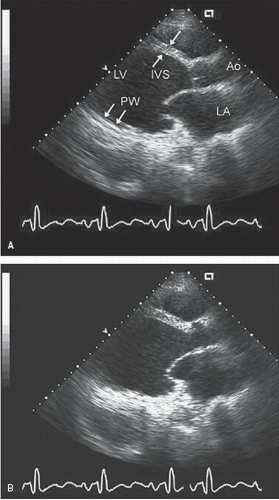 FIGURE 18.6. Parasternal long-axis view recorded in a patient with an ischemic cardiomyopathy. A: Recorded in end diastole. Note the dilated left ventricle and the relative preservation of ventricular septal thickness (upper arrows) as compared with the thinned posterior wall (PW) (lower arrows). B: End-systolic frame. Note the hypokinesis of the anterior septum and akinesis of the posterior wall. |
annulus of the heart toward the apex of ≥10 mm in normals. The magnitude of this motion can be determined with M-mode echocardiography or more recently has been evaluated using Doppler tissue imaging. In this technique, an M-mode cursor or a Doppler sample volume is placed in the lateral annulus or the proximal ventricular septum. The total excursion of the annulus toward the apex can then be measured (Fig. 18.9). For patients with global ventricular dysfunction, there is a direct relationship between annular excursion and left ventricular ejection fraction, such that the lower the systolic excursion, the lower the ejection fraction. This observation is only valid in the presence of global dysfunction.
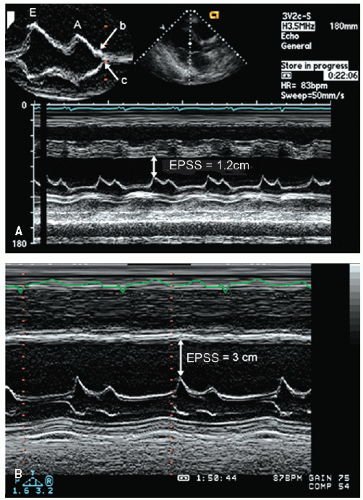 FIGURE 18.7. M-mode echocardiograms recorded in two patients with cardiomyopathy and systolic dysfunction. In each case, note the increased E-point to septal separation (EPSS) indicative of reduced ejection fraction. The EPSS is (A) 1.2 cm and (B) 3.0 cm. This suggests that the ejection fraction for the patient represented in B is substantially worse than that in A. The inset in A demonstrates a classic B-bump in mitral valve closure. Note that the smooth continuation between the A point and the closure point (c) is interrupted by transient reopening of the mitral valve denoted by the B-bump. |
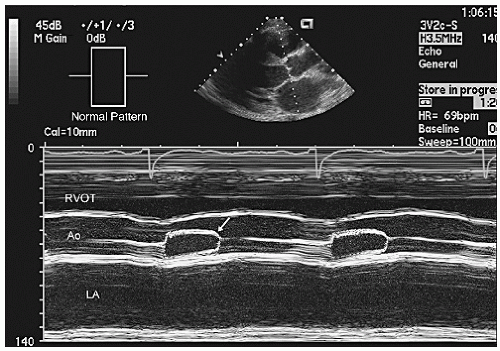 FIGURE 18.8. M-mode echocardiogram recorded through the aortic valve in a patient with a dilated cardiomyopathy and reduced stroke volume. Note the gradual curved closure of the aortic valve at end-systole (arrow). This is due to progressively diminishing forward flow as a consequence of severe systolic dysfunction. The small inset in the upper left schematizes the normal opening and closing pattern of the aortic valve. |
automatic edge detection algorithms, which may result in erroneous data in a poor-quality dataset where the entire endocardial border is not easily identified. Other newer techniques for quantifying systolic function include determination of regional or global strain with either Doppler tissue or speckle tracking algorithms (Fig. 18.12). Calculation of average or global strain throughout the entire perimeter of the left ventricle provides a parameter directly related to ejection fraction.
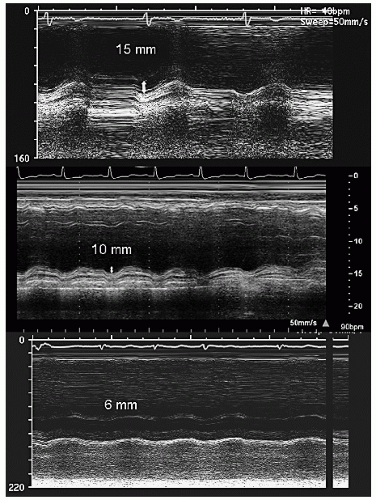 FIGURE 18.9. M-mode echocardiograms of the lateral mitral annulus recorded from the left ventricular apex. The top panel was recorded in a patient with normal ventricular function and annular excursion toward the apex is 15 mm. The middle panel was recorded in a patient with an ejection fraction of 42% and a dilated cardiomyopathy, note the annular excursion of 10 mm. The bottom panel was recorded in a patient with an ejection fraction of 21% and reveals annular excursion of 6 mm. |
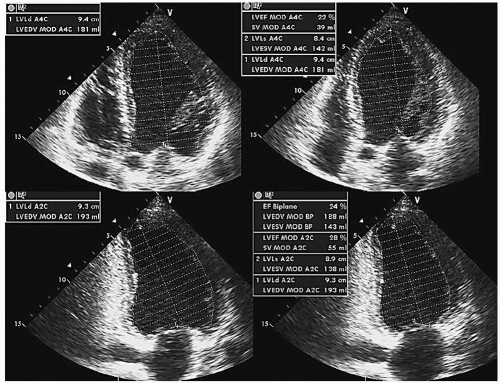 FIGURE 18.10. Apical four- and two-chamber views recorded in a patient with a nonischemic dilated cardiomyopathy from which diastolic (left panels) and systolic (right panels) frames have been used to calculate ventricular volumes using the rule of disks or Simpson’s method. The calculated volumes and subsequent ejection fraction for the four and two chamber as well as biplane methodology are as noted. |
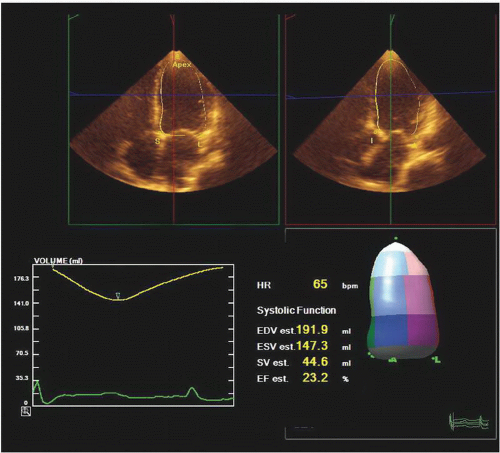 FIGURE 18.11. Calculation of end-diastolic volume (EDV) and end-systolic volume (ESV) in a patient using real-time three-dimensional echocardiography. The upper panels are the extracted four- and two-chamber views. The lower right is a shell based on the three-dimensional volume, from which EDV and ESV as well as stroke volume (SV) and ejection fraction (EF) are calculated. |
corresponds to clinical pulsus alternans, a sign of advanced ventricular dysfunction. Once per-beat stroke volume has been determined, cardiac output can be calculated as the product of the heart rate and forward stroke volume. This calculation assumes that aortic insufficiency is not present. The major source of error in this calculation is the measurement of left ventricular outflow tract area, which relies on the square of the radius. For any individual patient, one can assume the outflow tract area remains a constant, and, therefore, comparison of the TVI alone provides a reliable means for comparing the left ventricular stroke volume at different time points.
Table 18.4 Role of Doppler Echocardiography in Cardiomyopathy | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
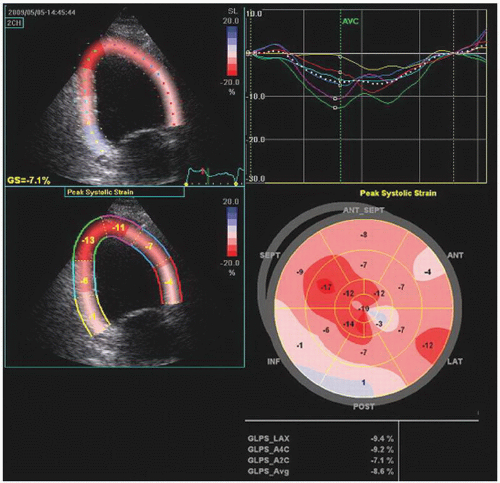 FIGURE 18.12. Tissue tracking performed for longitudinal strain in apical long-axis, four- and two-chamber views in a patient with a nonischemic dilated cardiomyopathy and ejection fraction of 23%. The data were extracted from a three-dimensional data set. The tissue tracking for longitudinal strain in the apical two-chamber view is presented along with the graphs of six individual segments in the upper right. The lower right is a bull’s eye diagram of peak systolic strain in all 17 segments. Global strain was -8.6%, which is reduced, and in line with the patients ejection fraction of 23%. Note in graphs of individual segments, the limited degree of dyssynchrony among segments based on the time to peak negative strain. AVC, aortic valve closure; GLPS, global longitudinal peak strain. |
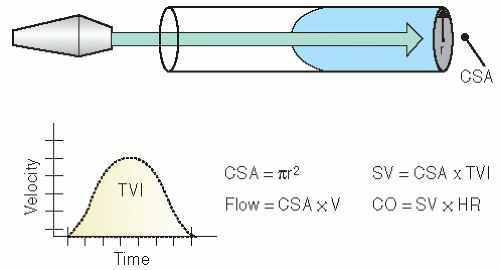 FIGURE 18.13. Schematic illustration outlining determination of stroke volume (SV) in the left ventricular outflow tract from which cardiac output (CO) can also be obtained. The crosssectional area (CSA) can be calculated from the outflow tract radius. Pulsed Doppler is used to determine the time velocity integral (TVI) of flow. Calculation of SV, flow, and CO are as noted. HR, heart rate. |
noninvasively determined dP/dt correlates well with values determined by cardiac catheterization, and dP/dt <600 mm Hg/sec has been associated with a worsened prognosis.
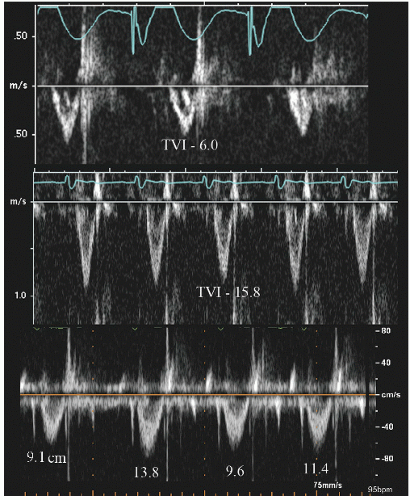 FIGURE 18.14. Left ventricular outflow tract time velocity integral (TVI) recorded in three patients with cardiomyopathy and reduced forward stroke volume. In the upper panel, note the marked decrease in TVI of 6.0 cm with less reduction in the middle panel. The bottom panel was recorded in a patient with severe left systolic dysfunction and reveals beat-to-beat variability in both the peak velocity and TVI which is a Doppler correlate of pulsus alternans, a clinical finding noted in advanced systolic dysfunction. |
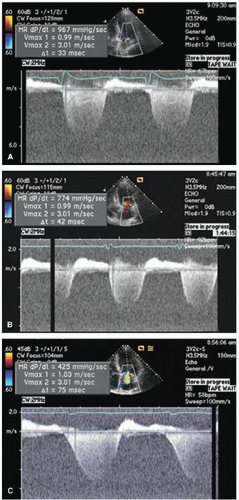 FIGURE 18.15. Examples of left ventricular dP/dt calculated from continuous wave Doppler of mitral regurgitation in three patients with dilated cardiomyopathy and varying degrees of left ventricular systolic dysfunction. A: Left ventricular dP/dt is relatively preserved at 967 mm Hg/sec. B, C: Moderate and marked reduction in left ventricular dP/dt is noted. |
dysfunction will have a pseudonormal pattern in which the mitral E/A ratio is normal in the presence of diastolic dysfunction. This pattern can be seen either as the patient progresses from mild diastolic dysfunction to more severe stages (grades 1 to 3 in Fig. 18.16) or as a patient is treated and has reduced left ventricular diastolic pressures and improves from grade 3 to 1. There are several ancillary measures that can help identify the pseudonormal pattern, including evaluating pulmonary vein flow, Doppler tissue imaging of the mitral annulus (Figs. 18.17 and 18.18), or reevaluating the mitral inflow pattern during the Valsalva maneuver. During the Valsalva maneuver, flow into the left heart is reduced and left atrial and ventricular diastolic pressure is decreased, resulting in a reduction in the E-wave velocity and reversal of the pseudonormal E/A ratio to reveal a pattern of abnormal relaxation (Fig. 18.19). As discussed in Chapter 7, these findings are accurate in the patient with systolic dysfunction but may not be relevant in disease-free individuals.
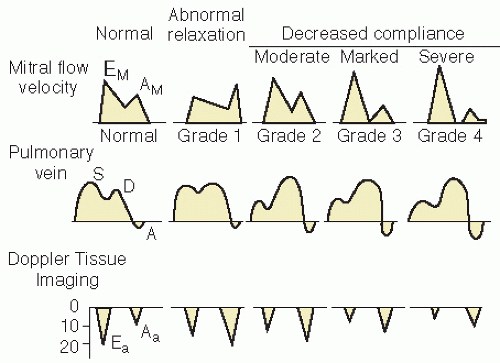 FIGURE 18.16. Schematic of different Doppler patterns seen in healthy subjects and patients with varying stages of diastolic dysfunction. Top: Mitral inflow recorded from the apex of the left ventricle. Middle: Pulmonary vein flow. Bottom: Doppler tissue imaging of the mitral valve annulus. The appearance of grade 4 dysfunction is similar to that of grade 3. Clinically, grade 4 is considered irreversible, whereas the grade 3 pattern may revert to grade 2 with maneuvers that reduce left ventricular filling acutely or after successful therapy. See text for further details. |
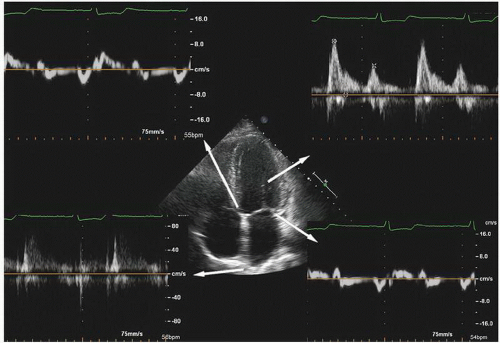 FIGURE 18.17. Echocardiographic images recorded in a patient with a dilated cardiomyopathy with an end-diastolic volume of 217 mL and an ejection fraction of 44%. The left atrium is dilated with a volume of 72 mL. Note the normal mitral valve E/A ratio but the reduced annular velocities and the blunted S wave of the pulmonary vein flow, all of which are consistent with diastolic dysfunction. |
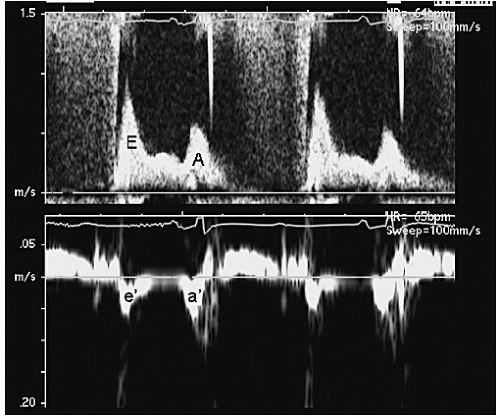 FIGURE 18.18. Mitral inflow pattern (A) and annular Doppler tissue imaging velocities (B) recorded in a patient with diastolic dysfunction. Note the normal mitral valve E/A ratio but the reduced e′/a′ ratio, implying diastolic dysfunction. In this example, the mitral E velocity is 90 cm/sec and the annular e′ velocity is approximately 5 cm/sec. The ratio E/e′ is 18, implying elevated left atrial pressure. |
mitral valve (E) to annular E velocity (e′) can be obtained (Figs. 18.18 and 18.20). This index (E/e′) has been reported to be linearly related to left atrial filling pressure. The majority of individuals with E/e′ >15 have elevated pulmonary papillary wedge pressures and individuals with E/e′ ≤8 generally have low left atrial filling pressures. E/e′ values between these values are associated with a broad range of filling pressures. This measure appears independent of heart rate and, because it relies only on early filling velocities, is also valid in patients with atrial fibrillation. Recent data have suggested that this relationship may be substantially less robust in clinical practice than initially reported, especially in patients with severe left ventricular dysfunction.
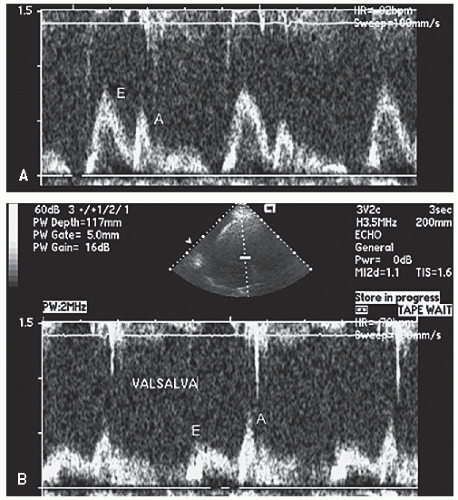 FIGURE 18.19. Effect of the Valsalva maneuver on the mitral inflow pattern in a patient with grade 2 diastolic dysfunction. A: Note the normal E/A ratio. During the Valsalva maneuver (B), left atrial and left ventricular filling is diminished and a reversed E/A ratio is uncovered. |
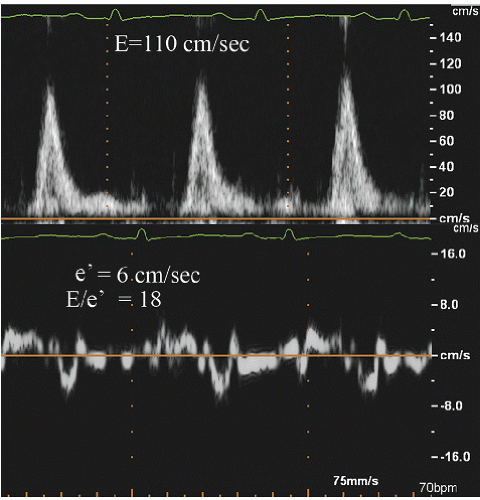 FIGURE 18.20. Mitral inflow and annular velocities recorded in a patient with an end-stage dilated cardiomyopathy. Note the E velocity of 110 cm/sec with an e′ of 6 cm/sec. E/e′ ratio is 18, suggesting elevated left atrial pressure. Also note the pathologically reduced systolic velocities of the mitral annulus. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


