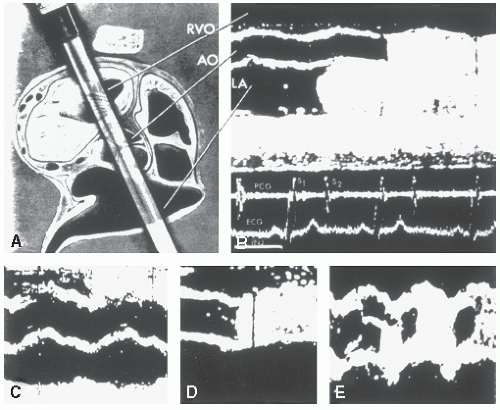
Ultrasound contrast agents were first used in conjunction with clinical echocardiography in the mid-1970s. Early agents consisted of either agitated saline or agitated saline stabilized with indocyanine green dye. Injections were done either intravenously or centrally at the time of cardiac catheterization. The resultant cloud of microbubbles was used to define cardiac borders and detect shunts. Early contrast echocardiography studies were essential for identifying the endocardial border and other structures with echocardiography (Fig. 4.1). After intravenous injection, these early contrast agents were isolated to the right heart and did not traverse the pulmonary circuit. As such, their appearance in the left heart was evidence of a right-to-left shunt.
Source of Ultrasound Contrast
Initial theories that the microbubble targets were created by cavitation at the time of injection have been dispelled. Although it is possible to create microbubbles due to a cavitation effect, the pressure with which fluid must be injected to create a cavitation effect is well beyond that encountered in routine clinical practice. Contrast occurring spontaneously at the time of an intravenous injection is more likely due to air contamination in the injection apparatus than to creation by the injection process.
Gas-containing microbubbles are intense ultrasound reflectors and reflect ultrasound at a level several orders of magnitude greater than non-gas-containing structures. Current ultrasound agents contain a variety of gases including air or, more recently, perfluorocarbons. It should be emphasized that the increased reflectivity from a microbubble target is due to the differential reflection of the contained gas compared with surrounding blood and tissue.
FIGURE 4.1. Early M-mode contrast echocardiograms recorded in the cardiac catheterization laboratory. A: The orientation of the M-mode ultrasound beam. B: Image was recorded after injection of contrast into the left atrium and shows subsequent appearance of contrast in the aorta. C: Contrast injected into the right ventricular outflow tract is shown. D: Contrast appears in the aorta after a left ventricular injection. E: Image was recorded after a supravalvular injection into the aorta. Contrast is seen exclusively in diastole with a contrast-free area due to competitive flow during aortic valve opening. (From Gramiak R, Shah PM, Kramer DH. Ultrasound cardiography: contrast studies in anatomy and function. Radiology 1969;92:939-948, with permission.) RVO, right ventricular outflow.
Contrast Agents
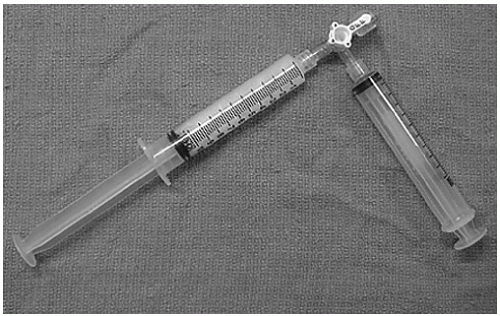
The simplest ultrasound contrast agent consists of saline microbubbles. Effective right heart contrast can be obtained by forcefully agitating a solution of saline between two 10-mL syringes, each of which contains 5 mL of saline and 0.1 to 0.5 mL of air (Fig. 4.2). Forceful agitation through a three-way stopcock creates a population of microbubbles that are highly variable in size and have a tendency to rapidly coalesce. After generation by agitation, they should be injected immediately to limit the time available for coalescence. These microbubbles, however, are intense echo reflectors and can be detected in the right atrium and right ventricle (Fig. 4.3). Their size precludes passage through the pulmonary capillary bed, and their appearance in the left heart implies a pathologic right-to-left shunt. By analyzing the timing and location of appearance, the nature of this shunt can often be determined as being a patent foramen ovale, atrial septal defect, or pulmonary arteriovenous malformation (AVM). Creation of ultrasound contrast by this technique is widely used in clinical practice and has an excellent safety profile.
Early attempts to create a more stable population of microbubbles involved reduction of surface tension. Surface tension increases the inward pressure of a bubble and is responsible for the tendency of a microbubble to collapse on itself. This tendency to spontaneously decrease in size due to surface tension results in a progressive increase in the pressure within the microbubble, which in turn increases the driving force for the contained gas to diffuse out of the bubble. These factors lead to an acceleration in the rate at which the microbubble shrinks and eventually disappears. By reducing and stabilizing surface tension, bubbles undergo less spontaneous collapse and a population of stabilized, longer lasting microbubbles can be created. Several agents including surfactant and indocyanine green dye have been used to reduce surface tension and create a population of smaller, more stable microbubbles. Many of the early fundamental observations in contrast echo were made using indocyanine green dye-stabilized microbubbles (Fig. 4.1). For practical purposes, there is little need to stabilize saline microbubbles. Because their size is relatively large, they do not pass the pulmonary capillary bed, and the safety record of this easily prepared agent has been remarkable.
FIGURE 4.2. Two-syringe and three-way stopcock apparatus for preparation of agitated saline contrast for intravenous injection. The total volume in the syringe on the left is approximately 10 mL, which consisted initially of 9.5 mL of saline and 0.5 mL of air. The contrast was prepared by forcefully injecting the solution from one syringe to the other through the three-way stopcock. Turbulence within the stopcock results in the creation of a large number of microbubbles that are suitable for intravenous injection. For opacification of right heart structures, a typical intravenous “dose” of contrast prepared in this manner ranges from 1.0 to 5.0 mL.
FIGURE 4.3. A: Apical four-chamber view recorded in a patient after injection of saline into a left upper extremity vein. B: After injection of intravenous contrast, there is uniform opacification of the right atrium and right ventricle with no appearance of contrast in the left heart, implying the absence of an intracardiac right-to-left shunt.
Beginning in the early 1980s, a number of attempts were made to engineer and manufacture microbubbles that would be uniform in size, have stability with respect to coalescence and size, and provide a homogeneous and reproducible degree of contrast. Recognition that high-intensity sonication resulted in populations of microbubbles was a major breakthrough in contrast echocardiography. The stability of the resultant contrast agent depended on the solution that was sonicated and the gas contained it. Through trial and error, it was recognized that sonication of 5% human albumin resulted in creation of a relatively homogeneous population of small microbubbles consisting of a denatured albumin shell containing air. These microbubbles were small enough to allow transpulmonary passage, resulted in an intense contrast effect, and could be commercially prepared as a sterile solution providing relating reproducible contrast effect. The major limitations of the early air-containing contrast agents were their relatively large size and inability consistently to pass through the pulmonary capillary bed in all patients. Refinements in the sonication process included replacement of the contained gas with a high-density perfluorocarbon instead of air and replacement of the albumin shell by a lipid membrane. A number of other approaches to the manufacture of microbubbles have also been undertaken including saccharide particles that form gas microbubbles on their surface and engineered microbubble shells of various size and composition. In general, the commercially available microbubbles have an initial size of 1.1 to 8.0 µm and are prepared at a concentration of 5 × 108 to 1.2 × 1010 microbubbles per milliliter. As such, the number of microbubbles injected per “dose” is substantially greater than that seen with agitated saline. Because of their stability (in a low ultrasound intensity field), they have substantial persistence, and a single injection will provide a usable contrast effect for 3 to 10 minutes.
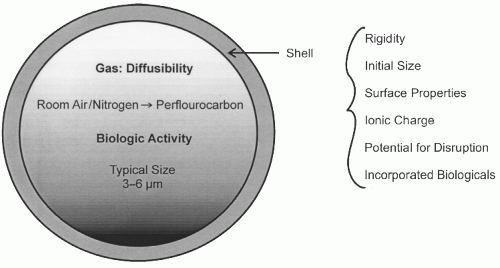
An engineered microbubble has two basic components, the outer shell and contained gas (Fig. 4.4). Bubble shells can be designed to be either rigid or flexible and to have varying resistance to collapse at high pressure. Recognition of these phenomena allows creation of microbubble populations that can be resistant to ultrasound destruction and, therefore, provide persistent contrast effect or can be easily destroyed by the ultrasound, resulting in simulated acoustic emission and enhanced detectability by this mechanism. The shell can be designed to allow varying degrees of permeability and outward diffusion of the contrast gas. Finally, the composition of the shell can be altered to include nonreflective therapeutic compounds. Some engineered microbubbles have shells which can be imbedded with specific antigenic binding sites, allowing them to be targeted to specific tissues. Application of the latter technology may allow delivery of chemotherapeutic or biologically active agents, including gene transfection vectors, to targeted tissue.
FIGURE 4.4. Schematic representation of a microbubble depicts its contents and various shell characteristics. See text for details.
The gas contained within the shell also affects the intensity and duration of the effect. Because the gas-blood interface is such a potent reflector, the intensity of contrast effect is substantially greater for any of the current generation of commercially available agents than that seen with agitated saline, largely because of the greater concentration of microbubbles. As is discussed subsequently, many ultrasound techniques either purposefully or incidentally disrupt the microbubble, allowing the gas to escape into the blood pool. Gases such as oxygen, nitrogen, and room air rapidly diffuse down a concentration gradient, resulting in rapid loss of contrast effect. High-density inert perfluorocarbons diffuse more slowly and, therefore, provide a longer lasting contrast effect even after bubble shell disruption.
Safety
In general, the perfluorocarbon-based commercially developed contrast agents have had a remarkable safety record. Until late 2007, there was little or no concern regarding their safety in a broad range of clinical situations. In October 2007, the U.S. Food and Drug Administration (FDA) issued a “black box” warning apparently intended as a class effect warning for commercially prepared contrast agents stipulating that they are contraindicated in pulmonary hypertension unstable cardiovascular situations, including arrhythmia, acute coronary syndrome, and congestive heart failure, and that 30 minutes of continuous electrocardiographic and hemodynamic monitoring was necessary after their administration. These warnings were based on four reported deaths in patients with significant underlying cardiovascular disease and unstable baseline status. These four deaths are out of an approximate 2 million exposures. After further review, the FDA revised its warning regarding contrast agents and limited the contraindications to patients with known right-to-left intracardiac shunts, known hypersensitivity to component agents including blood products or albumin (agent specific) as well as a continued nonapproval for intraarterial injection. Importantly, the requirement for 30 minutes of hemodynamic monitoring was removed from the vast majority of patients and now applies only to patients with unstable hemodynamics or arrhythmias who are likely to be studied in a monitored setting anyway. There have been four recent largescale surveillance studies, which have confirmed the safety profile of these agents (Table 4.1).
Multiple animal studies have been performed to evaluate the “dose response” of both contrast concentration and ultrasound delivery mode with respect to adverse effects. These studies have demonstrated the potential for creation of isolated ventricular arrhythmias as well as evidence of cellular damage related to contrast echocardiography when performed in higher than clinically relevant doses of the contrast agent and with algorithms for delivery of ultrasound exceeding those typically used in clinical practice. These studies suggest a substantial margin for safety of the agents when used as recommended according to clinical guidelines and also suggest parameters by which both the agent and the ultrasound instrumentation can be used for potentially therapeutic responses.
Clinical Use
The use of contrast echocardiography can be divided into five broad categories: (1) detection of intracardiac shunts, (2) left ventricular opacification for chamber delineation, (3) refined definition of left ventricular structural abnormalities, (4) myocardial perfusion, and (5) enhancement of Doppler signals. Detection of right-to-left shunts by detection of saline contrast in the left heart remains a primary use of contrast echocardiography. Left-to-right shunts can also be detected if a negative contrast effect is noted in the right heart. As noted elsewhere in this text, contrast echocardiography remains the standard for the diagnosis of a patent foramen ovale. This diagnosis is established using agitated saline, which does not pass through the pulmonary capillary bed as the contrast agent is cleared by the pulmonary capillaries. Because these newer agents cross the pulmonary capillary bed, their appearance in the left heart is not indicative of a pathologic shunt.
Because of their small size and stability, commercially available perfluorocarbon-based contrast agents pass through the pulmonary capillary bed relatively unimpeded and subsequently opacify the left ventricular cavity. This results in enhanced visualization of the left ventricular border and provides increased accuracy for border detection, chamber volume determination evaluation of regional wall motion, and evaluation of apical pathology. Even with the use of modern, high-frequency, short focal length transducers, specific apical pathology can occasionally be difficult to fully define. Opacification of the left ventricular cavity may allow further refinement in diagnosing apical pathology such as mural thrombus, apical hypertrophic cardiomyopathy, ventricular noncompaction, and rare, infrequent myocardial tumors.
The new contrast agents are also capable of opacification of the left ventricular myocardium. The appearance of contrast within the ventricular myocardium closely parallels the distribution of myocardial perfusion and experimentally has been used as a high resolution, nondestructive marker for evaluation of myocardial infarction. It should be emphasized that while myocardial perfusion contrast echocardiography has been shown to be feasible and accurate for identification of coronary stenosis in both animal and clinical studies, it is not currently approved for that purpose.
Finally, contrast agents can be used to enhance Doppler signals. This has had clinical utility for enhancing the tricuspid regurgitation signal for assessing right heart hemodynamics (saline contrast) and, less often, for enhancing a weak aortic stenosis jet or pulmonary vein flow signals. The use of contrast agents during color Doppler interrogation results in marked signal deterioration and is counterproductive.
Ultrasound Interaction with Contrast Agents
Microbubbles interact with the ultrasound beam in a variety of ways including direct reflection at the fundamental transmitted frequency and resonance with creation of reflected harmonic frequencies. The frequency at which a bubble has maximal reflectance is related to bubble diameter. For any ultrasound frequency, the amplitude of reflection from a microbubble decreases as the bubble diameter decreases. All bubbles have a diameter at which reflectance is maximal (the resonant diameter). Below the resonant diameter of the bubble, the amplitude of reflection again diminishes with the cube of the diameter. It is a fortuitous occurrence that bubbles having a diameter that allows transpulmonary passage have excellent reflectance when interacting with clinically relevant transmission frequencies.
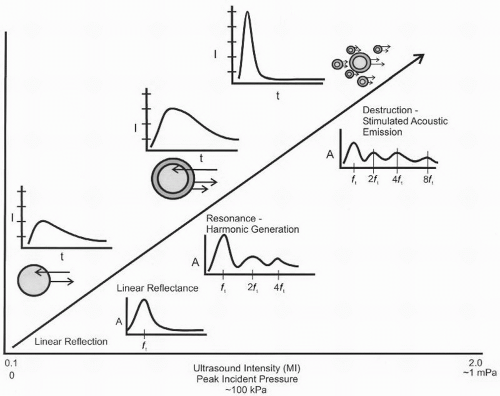
FIGURE 4.5. Schematic representation of various microbubble responses to increasing ultrasound intensity. Above the diagonal line, depicting increasing intensity, is a graphic representation of reflected image intensity at each level of ultrasound intensity and below the line a stylized depiction of the frequency response noted with each technique. At low intensity, a linear response can be obtained that results in detection of a returning frequency identical to the transmit frequency (ft). At higher incident pressures, bubble resonance occurs, resulting in the generation of a nonlinear or harmonic response such that signal is returned at the fundamental transmitted frequency as well as a series of its harmonics (e.g., ft). At higher ultrasound intensities, bubble integrity is disrupted resulting in a subpopulation of smaller bubbles with a broad range of resonant frequencies. Because bubble destruction occurs at the higher insonating pressure, the duration of contrast effect is substantially less.
Interaction of microbubbles with the ultrasound beam has three phases (Fig. 4.5). In its simplest form, ultrasound interacts with a microbubble by pure reflection of the ultrasound beam at its fundamental (i.e., transmitted) frequency. Maximal reflection from the microbubble is dependent on the relationship of the frequency and diameter as noted previously.
At higher ultrasound imaging intensities (typically ≥0.3 MI), microbubbles are not pure reflectors but begin to resonate. A resonating bubble will reflect ultrasound not only at the fundamental insonating frequency (ft) but also at harmonics of that frequency. In this instance, a microbubble insonated with a 2-MHz interrogating beam will reflect back the 2-MHz fundamental frequency but also resonate, creating reflected frequencies at 4, 8, and 16 MHz. Each of these subsequent harmonic frequencies doubles in frequency and diminishes in amplitude. In routine clinical practice, only the first harmonic (i.e., twice the fundamental frequency) is typically used for anatomic imaging. Contrast-specific imaging often relies on either multiple harmonic frequencies or subharmonics of the first harmonic (i.e., four and eight times the fundamental frequency). This provides a more contrast-specific signal.
At increasing ultrasound energy levels, the bubbles are physically destroyed by the insonating beam. The process of destruction results in the creation of subpopulations of bubbles of variable diameters. The highly variable diameter subpopulations result in a broad range of reflected frequencies. By this destructive bubble technique, a large amount of acoustic energy is generated both as reflected ultrasound and as multiple detectable Doppler shifts. This final phenomenon in which microbubbles are destroyed, thereby creating detectable ultrasound targets, is referred to as stimulated acoustic emission. This phenomenon can be maximized by the use of a microbubble with a fragile shell and containing nitrogen, or another rapidly diffusing gas, resulting in a rapid loss of the contrast effect after shell disruption.
Detection Methods
As noted above, interaction of microbubbles with ultrasound is complex and can be divided into three types of interaction: fundamental reflection, harmonic creation and detection, and stimulated acoustic emission. The receiving characteristics of the ultrasound instrument can be altered to capitalize on any of these three phenomena. Table 4.2 outlines the different ultrasound domains (e.g., B-mode vs. Doppler, etc.) and several commonly used acquisition modalities. Virtually, any of the different ultrasound domains can be linked to any of the acquisition methods to register the contrast-enhanced image. The exact combination of ultrasound domain and acquisition protocol will depend on the nature of the examination (e.g., left ventricular border vs. myocardial perfusion) as well as the characteristics of the available contrast agent and imaging platform.
Machine Settings
All current manufacturers provide dedicated contrast-specific presets to account for sensitivity of ultrasound contrast agents in a high-intensity field. Many of them have, as optional addons, contrast-specific modalities suitable for detection of lowintensity contrast in the myocardium. The users should be aware of the specific nature of the contrast presets, which are proprietary and vary from manufacturer to manufacturer and from platform to platform. Mechanical index (MI) is a measure of the power of an ultrasound beam and is defined as peak negative acoustic pressure/ft, where ft is the transmitted frequency. Routine B-mode scanning for anatomy and function typically is undertaken at a mechanical index of 0.9 to 1.4, which results in optimal tissue signature but substantial contrast destruction. Typically, at a mechanical index of 1.3 and above, all perfluorocarbon-based ultrasound contrast agents are rapidly destroyed in the ultrasound beam. Although this results in an instantaneous burst signal due to stimulated emission, the ongoing destruction of the agent results in the inability to detect any contrast effect. At a lower mechanical index (<0.3), continuous imaging of the blood pool-containing contrast can be undertaken with substantially less bubble destruction. This allows homogeneous detection of further contrast effect in the blood pool and to a lesser degree in the ventricular myocardium. General experience is that for use of contrast for left ventricular opacification, low mechanical index continuous imaging, often with phase analysis algorithms, will provide the optimal chamber opacification. Of note, these contrast-specific protocols inherent in modern platforms are not necessary when using agitated saline for detection of intracardiac shunts.
Table 4.2 Imaging Modalities for Contrast Detection
Ultrasound Domain
Acquisition Mode
B-mode
Continuous
Fundamental
Harmonic
Triggered
High mechanical index
Fixed interval
Low mechanical index
Variable, incremental interval
Triggered sequential
Doppler
Destruction/detection image sequence
Harmonic vs. fundamental
Frequency shift
Power spectrum
Correlation techniques
The simplest method for contrast detection is routine B-mode ultrasound. As noted previously, microbubbles are intense reflectors of ultrasound and the amount of reflected energy is substantially greater than that of the surrounding tissue or blood. Because of this, routine B-mode scanning is highly sensitive for the detection of isolated microbubble targets. This routine imaging technology is sufficient for detection of intracardiac shunts such as atrial septal defect using agitated saline. When used with newer perfluorocarbon-based agents, detection is markedly facilitated by the use of harmonic and other advanced imaging algorithms (Fig. 4.6).
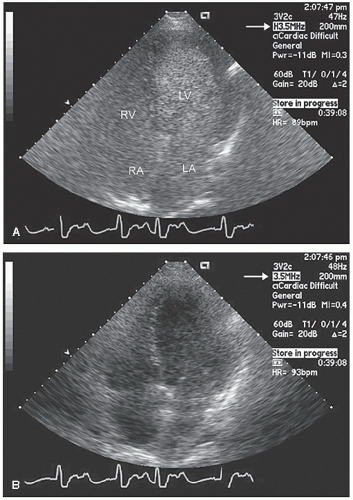
FIGURE 4.6. Four-chamber view recorded in a patient during harmonic (A) and fundamental (B) imaging. Note that with harmonic imaging, there is smooth opacification of the cavity and detection of contrast in all four cardiac chambers. Bottom: Recorded in the same patient using fundamental rather than harmonic imaging (arrows denote imaging mode). Note the lack of contrast detection with fundamental imaging.
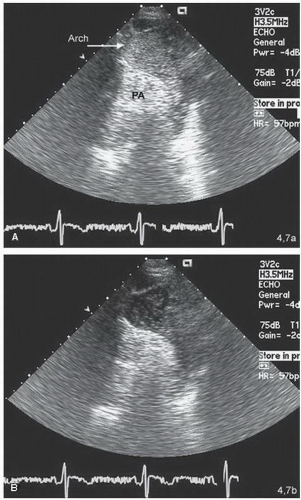
FIGURE 4.7. Suprasternal view of a normal aorta after intravenous injection of ultrasound contrast. The electrocardiogram is provided for timing. A: A systolic frame in which contrast is clearly identified in the arch of the aorta. B: The diastolic portion of the same cardiac cycle, in which far less contrast is detected, is shown. In the real-time image, note the phasic appearance and disappearance of the contrast in the aorta. Note that, during systole, a “fresh bolus” of contrast is ejected into the arch from an area out of the plane of imaging. During diastole, when there is less flow in the aorta, there is more time for ultrasound interaction with the contrast agent and it is progressively destroyed.
Intermittent Imaging
It was recognized in the mid-1990s that the routine interrogating ultrasound beam destroyed ultrasound targets (Figs. 4.7 and 4.8). This was a fortuitous observation made when investigators recognized the absence of contrast effect in the left ventricular cavity or myocardium during continuous imaging. After brief interruption of scanning, contrast was again detectable without reinjection of the agent. This led to the technique of intermittent imaging in which ultrasound interrogation is triggered to the electrocardiogram. In between triggered imaging, no ultrasound energy is delivered, allowing time for restitution of the contrast effect and its subsequent detection when imaging is resumed. Obviously, with intermittent imaging, the ability to analyze wall motion is lost, and this imaging technique is typically used for evaluation of myocardial perfusion. Similar studies also demonstrated a direct relationship between the microbubble destruction, measured as loss of contrast effect, and the intensity of delivered ultrasound (Fig. 4.8).
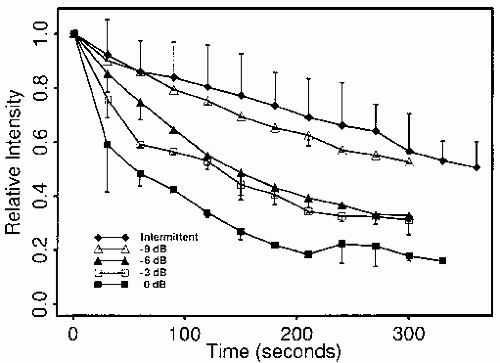
FIGURE 4.8. Impact of intermittent imaging and continuous imaging at four different ultrasound intensities in an in vitro model. Note the progressive decline in ultrasound contrast intensity with increasing ultrasound power from -9 dB to 0 dB. (Reprinted from Villarraga HR, Foley DA, Aeschbacher BC, et al. Destruction of contrast microbubbles during ultrasound imaging at conventional power output. J Am Soc Echocardiogr 1997;10:783-791, with permission).
Low Mechanical Index Imaging
Having recognized that the interrogating ultrasound beam is responsible for accelerated microbubble destruction and that continuous imaging results in the loss of contrast effect, algorithms for continuous imaging at a low mechanical index have been developed. Perhaps the single most important machine parameter to consider when using the modern generation of ultrasound contrast agents is the mechanical index. The mechanical index is a unitless number directly proportional to the power of the ultrasound beam being delivered. Typically, structural imaging without contrast enhancement will be undertaken at a mechanical index of 0.9 to 1.5. This degree of ultrasound delivery disrupts microbubbles and reduces the ability to use them clinically. As such, a mechanical index of ≥0.3 is typically employed for optimal detection of ultrasound within the left ventricular cavity or myocardium. By imaging at a low mechanical index, contrast within the left ventricular cavity is not destroyed, and because imaging is continuous rather than intermittent, wall motion analysis can be undertaken in real time with boundaries enhanced by the opacified left ventricular blood pool (Fig. 4.9). Low mechanical index imaging is also necessary when detecting very low concentrations of ultrasound contrast such as for myocardial perfusion. For myocardial perfusion imaging, intermittent high mechanical index imaging is often undertaken to purposefully destroy contrast in the blood pool to create a repeated bolus effect from which time appearance curves can be created.
Other Mechanical Factors Affecting Contrast Detection
In addition to mechanical index, there are other machine settings that have an impact on detection of ultrasound contrast. In general, anything that increases delivery of the ultrasound energy to the contrast agent results in a greater degree of destruction and consequently a decrease in the magnitude of contrast effect. As such, high frame rates will result in greater ultrasound contrast destruction than low frame rates. There can be selective destruction of contrast at the point at which a transmit focal zone has been set. Because of increased ultrasound energy at shallow imaging depths, the near field is more susceptible to contrast agent destruction than is the far field.
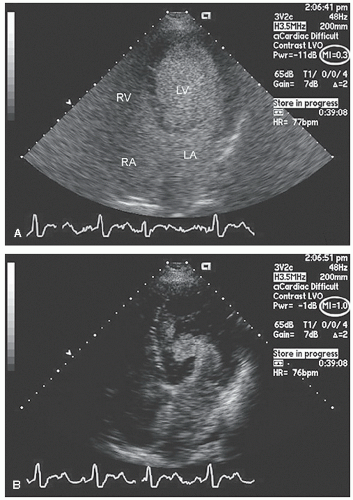
FIGURE 4.9. Apical four-chamber view recorded in a patient demonstrating the impact of mechanical index on contrast appearance. A: Image was recorded with a mechanical index of 0.3 and reveals smooth opacification of all four cardiac chambers. B: Image was recorded 10 seconds later with a mechanical index of 1.0. Note the complete lack of contrast in the near field and the swirling nature of the partial filling in the far field.
Doppler Imaging
Because bubbles interact with the ultrasound beam, they create a range of frequency shifts in the reflected beam that can be detected as a Doppler shift. These Doppler shifts are dependent not only on motion of the bubbles but also on their resonance in a stationary field. Within the Doppler domain, several parameters can be used to detect and quantify the contrast effect. Both the Doppler shift itself and the power of the Doppler spectrum, which is directly related to the number of targets being interrogated, can be registered and quantified. One of the more promising methods for detection of contrast effects is the use of phase correlation techniques, in which an automatic correlation of the insonating and reflected frequencies is undertaken. Because microbubbles are nonlinear reflectors and result in variable frequency shifts, the characteristics of reflected ultrasound from two sequential pulses will contain different reflected frequency spectra. This nonlinear response is not seen after interaction with tissue where the characteristics of two sequential ultrasound pulses will be identical. This methodology is referred to as phase image analysis. For phase image analysis two ultrasound signals are sent out with close temporal proximity (Fig. 4.10). The second pulse is 180° out of phase with the first pulse and may have a different amplitude. When the two reflected signals are then received, they are summed, and the summed ultrasound signal is then displayed. If each of these signals is reflected from a linear, nonharmonic reflector, such as tissue or blood, they are then received back at the transducer precisely 180° out of phase (exactly as transmitted), and when summed, they cancel each other to create zero signal. Conversely, if the signals interact with microbubbles, each signal is shifted in phase. Additionally, because microbubbles compress and expand at different rates in the ultrasound field, the contour of the reflected signal is altered compared with the transmitted signal. When summed, cancellation no longer occurs, and a signal is preserved. In theory, this provides a highly specific methodology for the detection of ultrasound contrast. This type of analysis is typically performed using the harmonic frequencies and provides a highly contrast-specific signal.
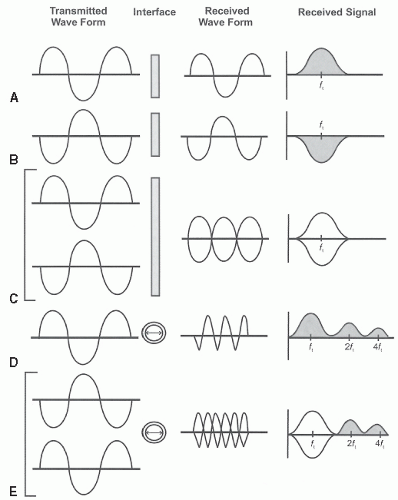
FIGURE 4.10. A simplified version of phase analysis is presented in which only sequential pulses 180° out of phase are diagrammed. In practice, both phase and amplitude may be altered in the sequential pulses. A: A transmitted wave interacts with a linear reflector (solid bar). The received wave is identical in configuration to the transmitted wave but will have less amplitude because of attenuation. The received signal is centered on the transmit frequency (ft). B: The identical frequency transmitted 180° out of phase with that in A. C: The interaction of two sequential pulses each of which is 180° out of phase with the other (A + B transmitted nearly simultaneously) is depicted. When received and summed, the waveform is as demonstrated and the received signal consists of identical positive and negative amplitudes that result in zero signal, as denoted by the absence of shading. D: The interaction of a transmitted wave with a microbubble is depicted. Because microbubbles contract and expand at different rates, they alter the contour of the transmitted wave. The received waveform has components of the fundamental frequency and harmonic frequencies at two and four times the transmit frequency. It is also altered in contour as noted. E: The interaction of two closely spaced pulses, 180° out of phase (identical to the transmitted pulses in C), which then interact with a microbubble is represented. Because the two pulses interact in opposite manners with the microbubble, they result in a more complex received waveform. The fundamental frequencies are returned 180° out of phase, and the harmonic signals are preserved. This results in a relatively contrast-specific signal.
Contrast Artifacts
Appropriate and successful use of ultrasound contrast requires careful attention to technical detail and machine and imaging algorithms that often differ from those used for routine clinical scanning. Even with meticulous attention to detail, there are a number of pitfalls and artifacts that can diminish the clinical yield of contrast echocardiography. Contrast artifacts can be divided into two broad categories: those due to the agent and its interaction with the ultrasound beam, and physiologic artifacts, both of which may interfere with interpretation (Table 4.3).
Table 4.3 Contrast Artifacts
Agent/ultrasound related
Attenuation
Shadowing
Apical destruction
Physiologic
Competitive flow
SVC—IVC
Marginated flow
Incomplete blood pool mixing
Eustachian valve
IVC, inferior vena cava; SVC, superior vena cava.
As contrast agents are very potent reflectors of ultrasound, their presence in high concentration results in nearly complete attenuation of ultrasound penetration. This phenomenon is particularly prominent when using the newer, more highly reflective perfluorocarbon-based agents. Attenuation occurs when there is an abnormally high concentration of ultrasound targets in the near field, beyond which the ultrasound beam cannot penetrate (Figs. 4.11 and 4.12). This results in detection only of the initial layer of contrast-enhanced blood, with all areas of the heart behind this area being shadowed. Attenuation is common during bolus injections of perfluorocarbon-based agents. It can be avoided by delaying scanning until later in the infusion protocol, after the peak contrast effect has declined, or preferably by the use of a smaller bolus or lower concentration of the ultrasound agent. Clinically, the attenuation phenomenon is most problematic when imaging the basal lateral wall in an apical four-chamber view. This region is often an area of contrast dropout which should not be confused for the ventricular boundary, either for wall motion analysis or for volumetric determination. Similarly, this area of greatest attenuation can be remarkably problematic for assessing myocardial perfusion.
Only gold members can continue reading. Log In or Register to continue