Table 20.1 Indications for Echocardiography in the Adult Patient with Congenital Heart Diseasea | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
Table 20.2 A Segmental Approach to Cardiac Situs and Malpositions | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||
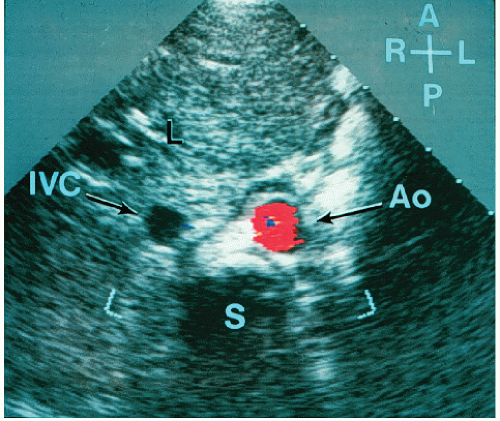 FIGURE 20.1. Subcostal short-axis view of the subject with situs solitus. The liver (L) and inferior vena cava are on the patient’s right, and the aorta is to the patient’s left. With the use of color flow imaging, flow within the aorta is detected. A, anterior; I; L, left; P, posterior; R, right; S, spine. |
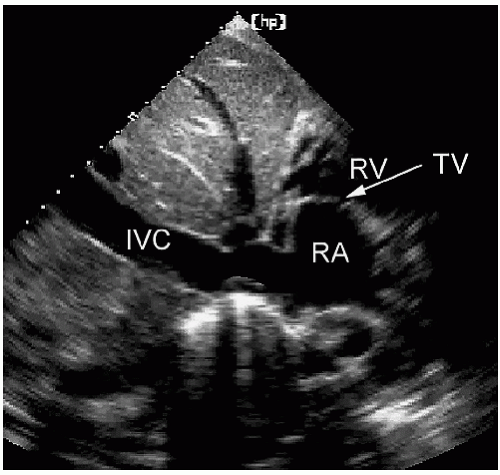 FIGURE 20.2. Subcostal long-axis view of a normal subject. The inferior vena cava can be seen entering the right atrium. TV, tricuspid valve. |
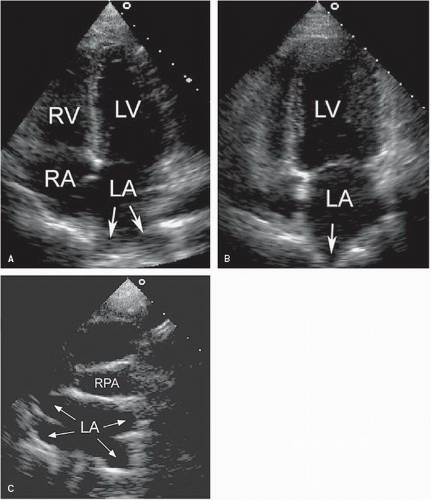 FIGURE 20.3. Apical four- (A) and two-chamber (B) views from a patient demonstrate the entrance of the pulmonary veins (arrows) into the left atrium. C: A suprasternal short-axis view shows the posterior region of the left atrium, below the right pulmonary artery (RPA), where the pulmonary veins enter (arrows). |
atrioventricular valves associate with the corresponding ventricle and identification of the mitral and tricuspid valves defines the respective chambers. The tricuspid valve is more apically displaced and has three leaflets (and three papillary muscles) and chordal insertions into the septum. The mitral valve has a more basal septal attachment and has two leaflets, which insert into two papillary muscles but not the septum. All these features can be assessed with echocardiography. The four-chamber view allows the echocardiographer to determine ventricular morphology and the relative positions of the atrioventricular valves. The short-axis views permit definition of the papillary muscles and chordal insertions. The relative positions of the atrioventricular valves and the presence or absence of chordal insertions into the septum are the most helpful echocardiographic features when attempting to determine ventricular identity.
Table 20.3 Echocardiographic Characteristics of Right and Left Ventricles | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
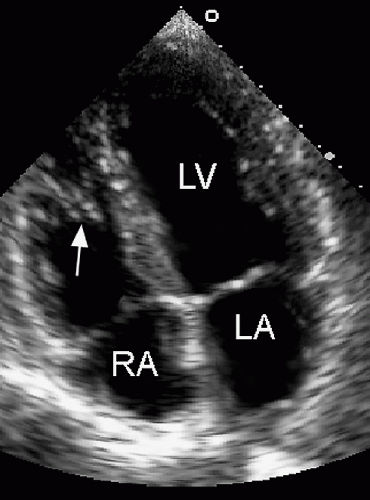 FIGURE 20.4. Apical four-chamber view from a healthy subject with a prominent moderator band (arrow), which represents a normal structure that is occasionally confused with thrombus or tumor. |
assessing from the suprasternal short-axis view the course of the brachiocephalic vessels as they leave the arch.
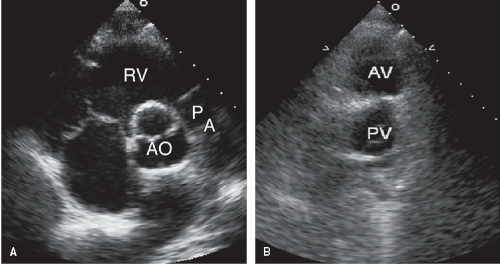 FIGURE 20.5. Parasternal short-axis echocardiograms from a healthy subject (A) and a patient with D-transposition of the great arteries (B). In the healthy subject, the aortic valve (AV) is posterior and the right ventricular outflow tract and pulmonary artery (PA) appear to wrap around the aorta. With transposition, the aorta is anterior and the two great vessels arise in parallel. PV, pulmonary valve. |
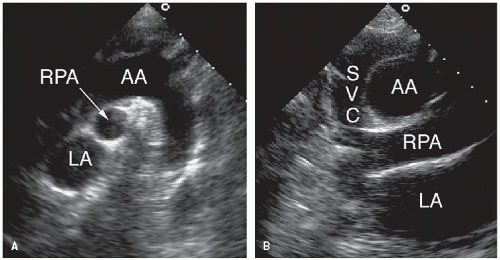 FIGURE 20.6. Suprasternal long- (A) and shortaxis (B) views from a healthy subject. The right pulmonary artery (RPA) passes below the aortic arch (AA) and above the left atrium. The superior vena cava can be seen to the right of the aortic arch. |
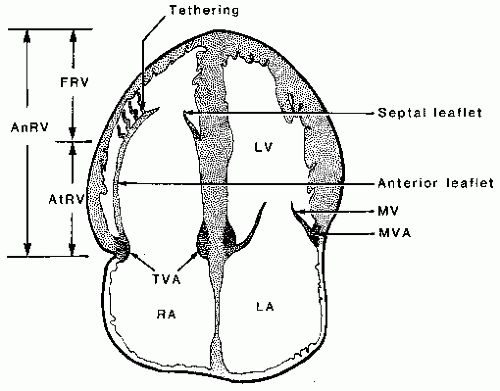 FIGURE 20.7. Schematic of anatomic abnormalities in Ebstein anomaly. AnRV, anatomic right ventricle; AtRV, atrialized right ventricle; FRV, functional right ventricle; MV, mitral valve; MVA, mitral valve annulus; TVA, tricuspid valve annulus. |
investigators have advocated a maximal displacement of more than 20 mm as the diagnostic criterion in adults.
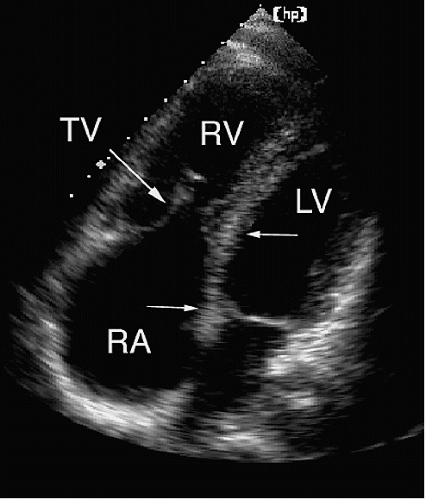 FIGURE 20.8. A four-chamber view from a patient with Ebstein anomaly. The arrows indicate the degree of apical displacement of the tricuspid valve (TV), which had restricted motion. Note that the functional portion of the right ventricle is fairly well preserved. |
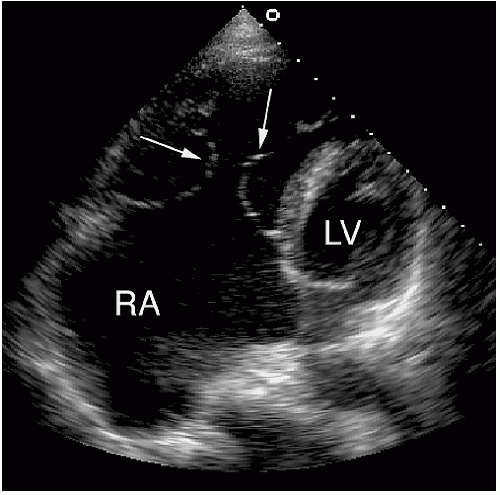 FIGURE 20.9. A more extreme form of Ebstein anomaly. The tricuspid valve (arrows) is markedly abnormal, and there is tethering of the leaflets, which prevented normal coaptation and resulted in significant tricuspid regurgitation. The right atrium is severely dilated. |
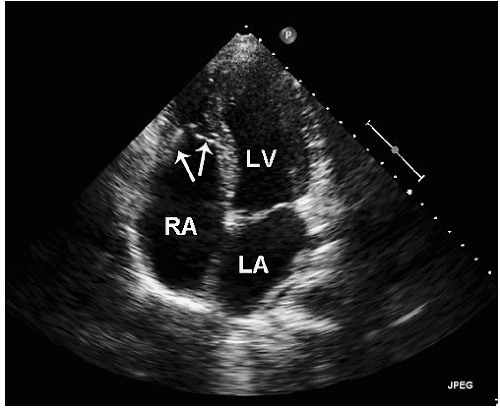 FIGURE 20.10. An example of Ebstein anomaly. From the apical four-chamber view, the tricuspid valve leaflets (arrows) are displaced far into the right ventricular apex. |
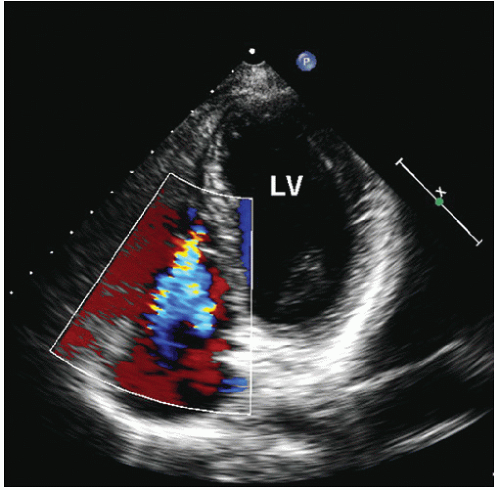 FIGURE 20.11. Color flow imaging is used to demonstrate tricuspid regurgitation in the setting of Ebstein anomaly. |
the transducer to the left atrium, transesophageal echocardiography is superior for recording the insertion of the pulmonary veins (Fig. 20.12A). An approach to pulmonary vein visualization using this technique is covered in detail in Chapter 8. In most patients, all four veins can be visualized. Echocardiography has also been used for the diagnosis of pulmonary vein obstruction from compression by an extrinsic mass or secondary to stricture after an atrial fibrillation ablation procedure.
Table 20.4 Levels of Obstruction of Left Ventricular Inflow | |||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||
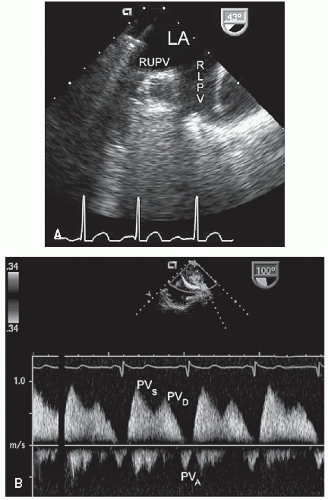 FIGURE 20.12. A: A transesophageal echocardiogram shows the entrance of the right lower pulmonary vein (RLPV) and the right upper pulmonary vein (RUPV) into the left atrium. B: Flow in the left upper pulmonary vein is recorded from transesophageal echocardiography. In this example, moderately increased flow velocity is the result of left-to-right shunting through an atrial septal defect. PVS, PVD, and PVA refer to pulmonary vein flow during systole, diastole, and atrial systole, respectively. |
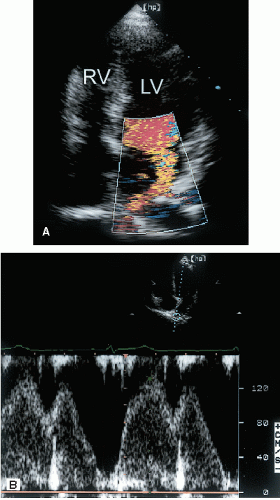 FIGURE 20.13. A patient with pulmonary vein stenosis. A: Color Doppler imaging demonstrates a turbulent jet that appears to originate from the right upper pulmonary vein as it enters the left atrium. B: Pulsed Doppler imaging reveals nearly continuous antegrade flow and increased velocity. |
the atrial appendage and mitral valve (which is usually normal). Because of the orientation of the membrane, the four-chamber view is often optimal because it places the membrane perpendicular to the beam. Note in Figure 20.14 the improved visualization of the membrane from an apical window compared with the parasternal view. The obligatory perforation connecting the two is most often posterior and may be multiple. This communication may be difficult to record with echocardiography. Color Doppler imaging usually permits localization of the opening in the membrane so that the pressure gradient can be assessed with pulsed Doppler imaging (Fig. 20.15). When the transthoracic study is suboptimal, transesophageal echocardiography should be used for evaluating this entity. Figure 20.16 is an example of cor triatriatum assessed from the transthoracic approach. The atrial membrane is clearly visualized from multiple views.
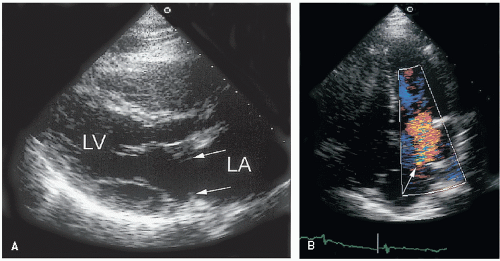 FIGURE 20.14. Cor triatriatum is demonstrated from the parasternal long-axis (A) and fourchamber (B) views. The membrane (arrows) within the left atrium is much better seen from the apical window. In such cases, color Doppler imaging is useful to demonstrate turbulent flow through the defect in the membrane (arrow). |
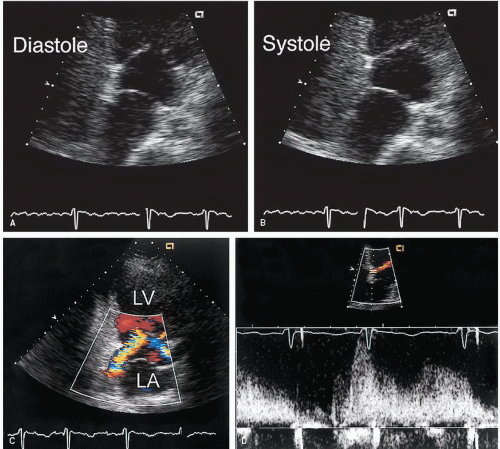 FIGURE 20.15. An example of cor triatriatum. The diastolic frame (A) and systolic frame (B) demonstrate the relationship of the membrane to the mitral valve. C: Color Doppler imaging reveals the perforation within the membrane and the turbulent flow into the lower portion of the left atrium. D: Pulsed Doppler imaging is used to assess flow velocity across the membrane, which has an appearance similar to that of mitral stenosis. |
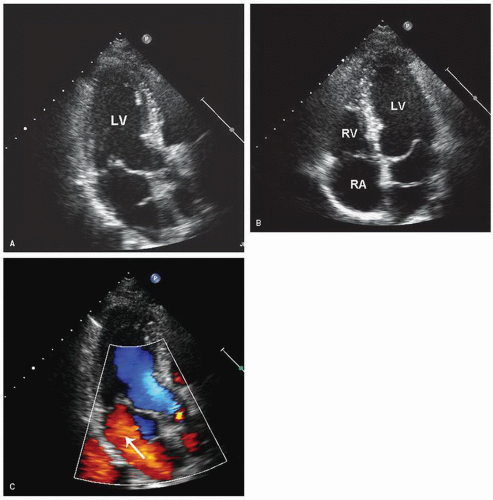 FIGURE 20.16. In this patient with cor triatriatum, the linear echo seen within the left atrium represents a membranous partition in the chamber. This membrane is visualized from the apical long-axis (A) and the four-chamber view (B). In panel C, color flow imaging demonstrates left atrial flow around the membrane and through the mitral valve, confirming incomplete partitioning of the atrium. |
turbulence at the level of the annulus rather than the leaflet tips is an additional clue to distinguish a supravalvular ring from mitral valve stenosis. Continuous wave Doppler imaging can then be used to assess the severity of the obstruction (see Fig. 20.17D). The proximity of the membrane to the valve can lead to leaflet damage, the result of high-velocity turbulent flow. Leaflet thickening and mitral regurgitation may develop as a consequence. Caution must be used when diagnosing a supravalvular stenosing ring with echocardiography. Differentiating between a thickened and calcified mitral annulus and a stenosing ring may be difficult, leading to both false-positive and false-negative results. Associated anomalies are seen frequently with both cor triatriatum and supravalvular stenosis. Atrial septal defect and persistent left superior vena cava are especially common and are readily detected with echocardiography.
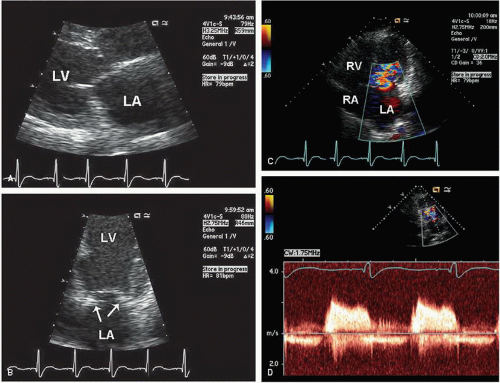 FIGURE 20.17. An example of Shone’s complex. A: Restricted mitral valve motion during diastole is present, but the stenosing ring is not visualized from this view. B: The restricted leaflet motion, as well as the presence of the fibrous ring (arrows) and its relationship to the mitral valve, is better seen from the apical four-chamber view. C: Color Doppler imaging demonstrates turbulent antegrade flow during diastole through the abnormal mitral valve. D: Continuous wave Doppler imaging demonstrates a significant pressure gradient across the mitral valve. |
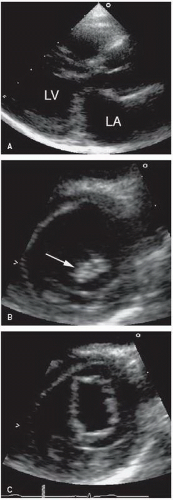 FIGURE 20.18. An example of parachute mitral valve. A: The long-axis view reveals thickened mitral leaflets that dome in diastole. B: A short-axis view at the midventricular level demonstrates the chordae converging on a single papillary muscle (arrow). C: The orifice of the abnormal mitral valve is shown from the short-axis view. Although the orifice is large, a mild degree of subvalvular gradient was present. |
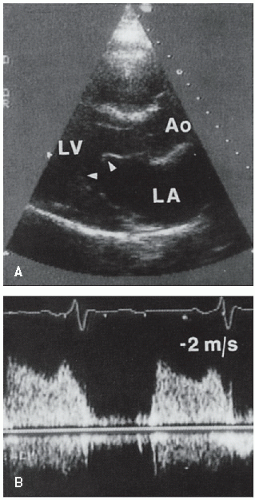 FIGURE 20.19. Parasternal long-axis view (A) and continuous wave Doppler recording of mitral inflow (B) from a child with a parachute mitral valve. The echocardiogram reveals a thickened mitral valve with restricted leaflet mobility and chordal fusion (arrowheads). The left atrium is dilated. Color flow imaging revealed a turbulent and anteriorly directed jet. Continuous wave Doppler imaging demonstrates significantly increased inflow velocity and a prolonged pressure half-time consistent with mitral stenosis. |
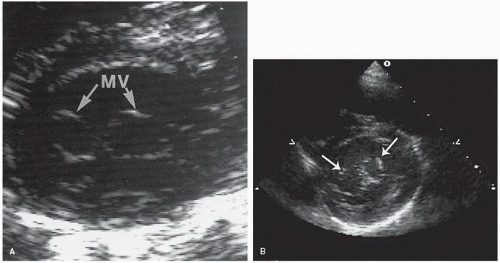 FIGURE 20.20. Parasternal short-axis views from two patients with double-orifice mitral valve (MV). |
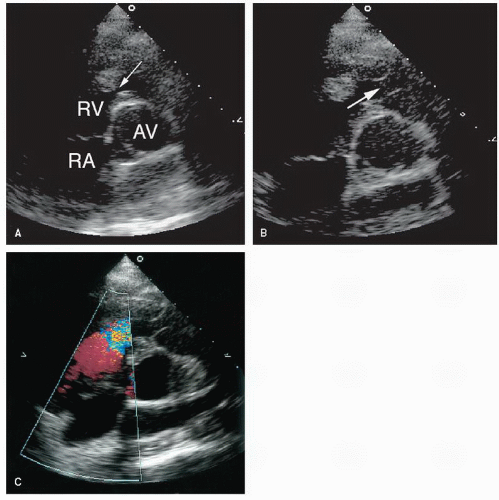 FIGURE 20.21. A series of short-axis images demonstrate infundibular right ventricular narrowing. A: Note the presence of muscle bundles in the area of the right ventricular outflow tract (arrow). B: The relationship of the subvalvular narrowing to the pulmonary valve (arrow). C: Color Doppler imaging demonstrates turbulence in this area. Dynamic subvalvular stenosis is present with a late-peaking gradient. AV, aortic valve. |
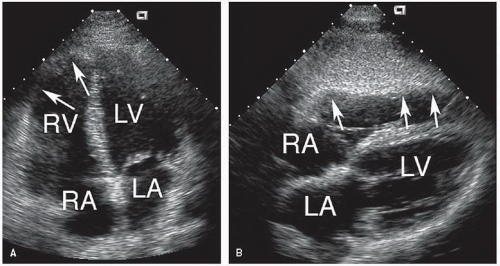 FIGURE 20.22. Extensive right ventricular involvement in a patient with arrhythmogenic right ventricular cardiomyopathy/dysplasia. A: The apical four-chamber view demonstrates dilation of the right ventricle and hypokinesis of the right ventricular free wall (arrows). B: A subcostal view reveals segmental right ventricular dysfunction in some aneurysmal dilation near the apex (arrows). |
of the lesions. Proximal lesions can be visualized from the parasternal short-axis window. Figure 20.27 is an example of peripheral pulmonary stenosis involving the right branch. In most such cases, the diagnosis is apparent from twodimensional echocardiographic imaging. Color Doppler imaging should be used to demonstrate turbulence and acceleration of flow within the stenotic segment. The echocardiographer must bear in mind, however, that a more common cause of turbulent flow within the main pulmonary artery is patent ductus arteriosus. More peripheral stenoses may be impossible to visualize, especially in older patients. In children, the subcostal four-chamber and the suprasternal views may permit detection of distal lesions. The diagnosis should be considered in a patient with unexplained right ventricular hypertrophy, particularly in the presence of a pulsatile proximal pulmonary artery.
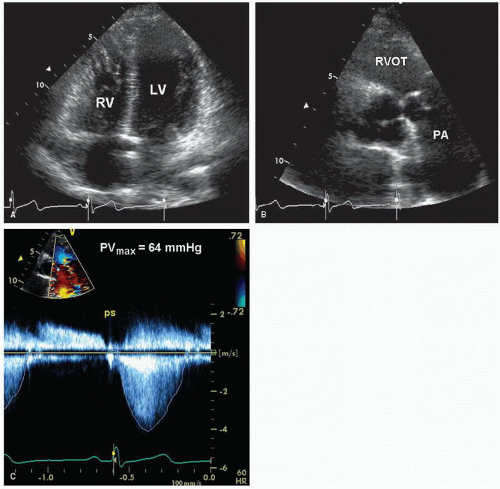 FIGURE 20.23. An example of valvular pulmonary stenosis. A: From the four-chamber view, the right ventricle is hypertrophied with normal systolic function. B: A basal short-axis view demonstrates doming and mild thickening of the pulmonary valve. C: Doppler imaging demonstrates a peak gradient of 64 mm Hg. AV, aortic valve; PA, pulmonary artery. |
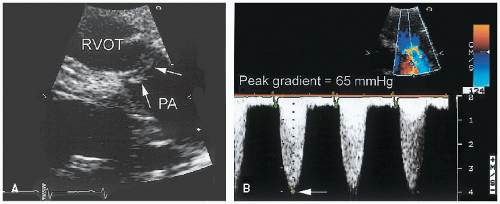 FIGURE 20.24. An example of dysplastic pulmonary valve stenosis. A: The pulmonary valve (arrow) is markedly thickened and immobile. Doming during systole is present. B: A maximal pressure gradient of approximately 65 mm Hg. PA, pulmonary artery. |
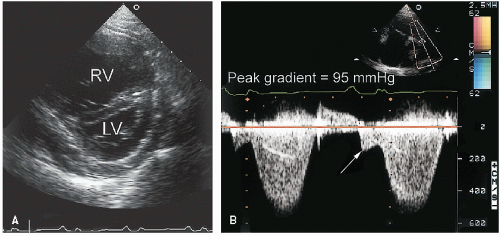 FIGURE 20.25. A: A patient with severe pulmonary stenosis demonstrates septal flattening with a dilated and hypertrophied right ventricle. These findings are consistent with right ventricular pressure overload. B: Severe pulmonary stenosis is confirmed with a maximal pressure gradient of approximately 95 mm Hg. Note the presence of presystolic flow through the pulmonary valve at the time of right atrial systole (arrow). |
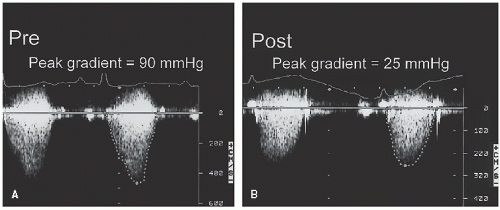 FIGURE 20.26. A case of pulmonary stenosis is shown before (Pre) (A) and after (Post) (B) valvuloplasty. The procedure resulted in a decrease in pulmonary valve gradient from 90 to 25 mm Hg. |
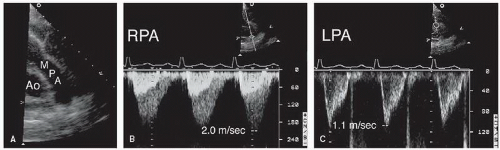 FIGURE 20.27. An example of pulmonary artery stenosis. A: The main pulmonary artery (MPA) appears normal. B: Flow through the right pulmonary artery (RPA) demonstrates increased velocity and acceleration. C: Normal flow velocity through the left pulmonary artery (LPA). |
all cases of left ventricular outflow obstruction in children and both are uncommon in adult patients. Discrete subaortic stenosis results from a thin, fibrous membrane or ridge that forms a crescentic barrier within the outflow tract just below the aortic valve. The membrane usually extends from the anterior septum to the anterior mitral leaflet. The degree of obstruction to flow is variable, and aortic regurgitation develops in approximately 50% of patients. With two-dimensional echocardiography, these membranes are seen as a discrete linear echo in the left ventricular outflow tract perpendicular to the interventricular septum. Because the membranes are parallel to the beam, recording these structures from the parasternal long-axis window may require the use of multiple transducer positions (Fig. 20.28). In many cases, the membranes are detected more easily from the apical views (where the ultrasound beam is oriented perpendicular to the structure) (Fig. 20.29). Transesophageal echocardiography has also been used in the assessment of patients with subvalvular obstruction. Doppler imaging plays an essential role in the evaluation of these patients. After the location and orientation of the jet are visualized with color flow imaging, continuous wave Doppler imaging can be used to estimate the peak pressure gradient across the membrane (Fig. 20.30). In the absence of aortic valve stenosis, this value correlates well with the catheterization-derived measure of obstruction. In the presence of multiple serial stenoses, however, Doppler imaging may overestimate the catheterizationmeasured gradient. The presence and severity of aortic regurgitation can also be assessed with Doppler techniques (Fig. 20.28). Figure 31 is an example of a subaortic membrane evaluated with transesophageal imaging. Note how the attachment of the membrane to the anterior mitral leaflet deforms the valve, especially during systole. M-mode echocardiography can also be helpful in assessing subvalvular obstruction (Fig. 31C). Midsystolic partial closure with reopening of the leaflets in late systole is indicative of a subvalvular pressure gradient.
Table 20.5 Classification of the Various Congenital Forms of Left Ventricular Outflow Tract Obstruction | ||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||
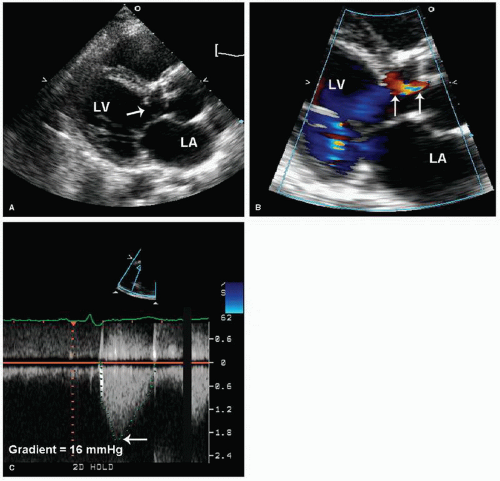 FIGURE 20.28. An example of subvalvular membranous aortic stenosis. A: The location of the membrane (arrow) and its proximity to the aortic valve is demonstrated from the parasternal long-axis view. B: As is often the case, some degree of aortic regurgitation is present as indicated by the white arrows. C: Doppler imaging demonstrates a peak gradient 16 mm Hg, excluding a significant degree of obstruction. |
 FIGURE 20.29. A: A subaortic membrane is readily apparent in this apical four-chamber view. B: The presence of the membrane results in turbulence in the left ventricular outflow tract, proximal to the aortic valve. This high-velocity, turbulent flow can result in damage to the aortic cusps. |
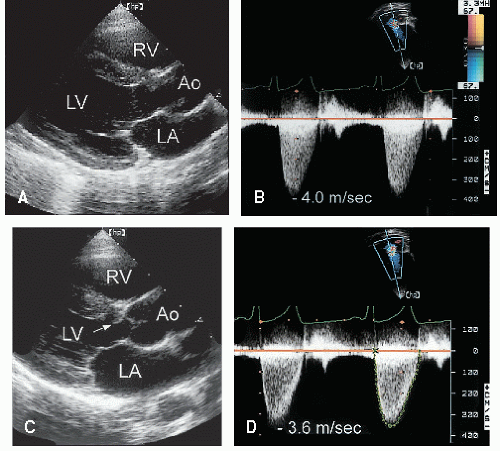 FIGURE 20.30. These two cases demonstrate the continuum between a discrete subaortic membrane and a fibromuscular ridge. A: A discrete membrane is demonstrated. Note how the membrane attaches to and deforms the base of the anterior mitral leaflet. A 60 mm Hg peak systolic gradient is confirmed (B). C: A fibromuscular ridge (arrow) in association with a membrane is located just below the aortic valve. In this patient, the peak gradient across the subvalvular obstruction is approximately 52 mm Hg (D). |
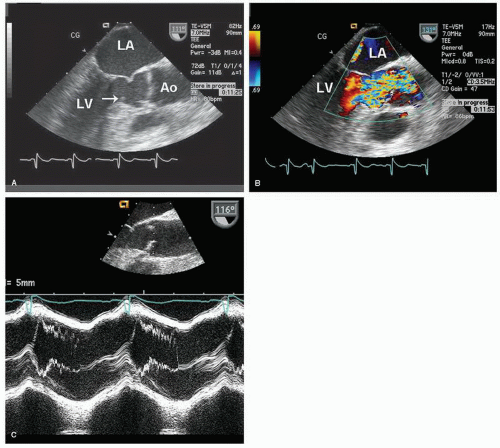 FIGURE 20.31. A subaortic membrane is demonstrated using transesophageal echocardiography. A: From a long-axis view, the membrane can be seen in the left ventricular outflow tract extending from the septum (arrow) to the anterior mitral leaflet. Note how the mitral leaflet is deformed by the attachment of the membrane. B: Color Doppler during systole demonstrates turbulent flow within the left ventricular outflow tract, beginning at the level of the membrane. C: With a subaortic membrane, M-mode echocardiography demonstrates the characteristic midsystolic partial closure and coarse fluttering of the aortic valve cusps. |
distinct sinuses will establish this difference. Confirming the presence of a bicuspid aortic valve with echocardiography requires high-resolution images from the short-axis view for adequate visualization of valve morphology. A unicuspid valve has a single slitlike commissure, and the opening is eccentric and restricted. The stenotic tricuspid valve has three cusps with variable degrees of commissural fusion. Thus, an accurate assessment of functional anatomy requires an analysis of the number of apparent cusps, the degree of cusp separation, and a recording of their mobility and excursion during systole.
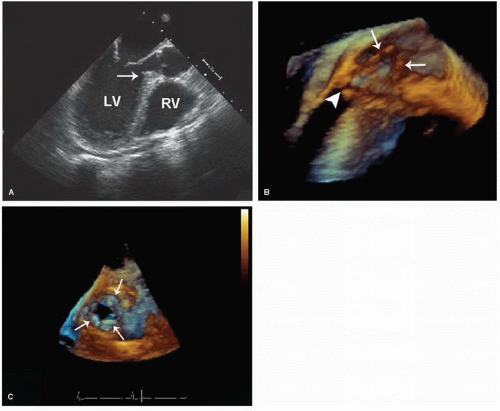 FIGURE 20.32. A transesophageal echocardiogram, using both two-dimensional and three-dimensional imaging, is recorded in a patient with a fibromuscular ridge. A: In the long-axis view, fibrous thickening of the basal septum, just below the aortic valve is indicated by the arrow. B: The same long-axis view is shown using three-dimensional imaging. The relationship between the aortic cusps (arrows) and the narrowed outflow tract (white arrowhead) is demonstrated. C: Recorded from a short-axis view just above the aortic valve, this three-dimensional echocardiogram illustrates the subaortic orifice located just below the aortic cusps (indicated by the three white arrows). |
principles underlying these applications are covered in detail in Chapters 9 and 11.
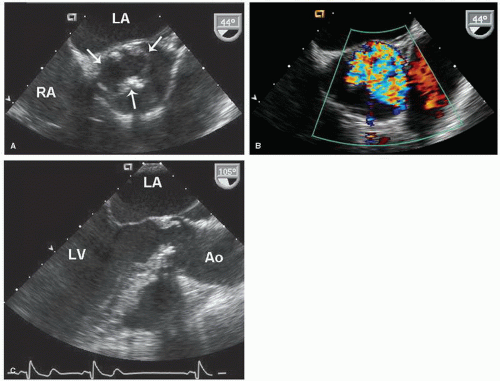 FIGURE 20.33. A unicuspid aortic valve is evaluated with transesophageal echocardiography. A: From a short-axis view, the eccentric, oval-shaped orifice is shown during systole (arrows). B: Color flow imaging demonstrates turbulent, eccentric antegrade flow. C: From a long-axis view, the systolic doming of the aortic valve is apparent. |
peripheral pulmonary stenosis may be inherited as an autosomal dominant trait.
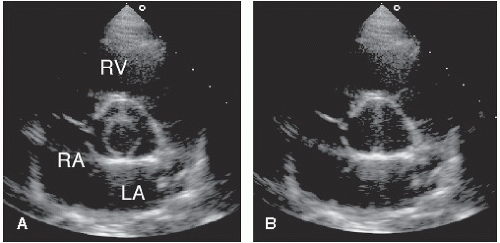 FIGURE 20.34. A bicuspid aortic valve is demonstrated from the short-axis view. The systolic frame (A) demonstrates a circular orifice. B: During diastole, a vertical commissure is seen between the two cusps. |
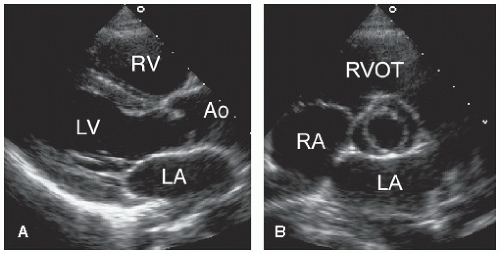 FIGURE 20.35. A functionally normal bicuspid aortic valve from a young patient. A: Long-axis view demonstrates doming of the valve in systole. B: Basal short-axis view confirms that the valve is bicuspid but with no evidence of stenosis. |
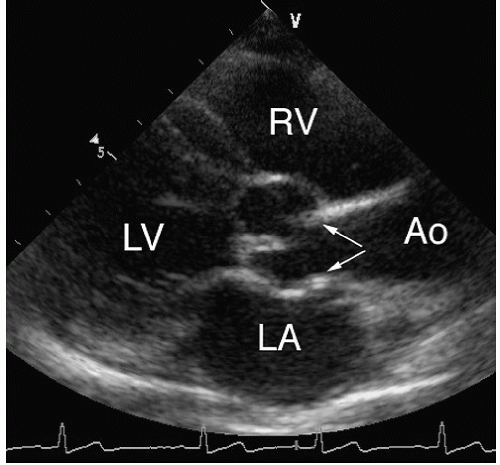 FIGURE 20.36. A child with supravalvular aortic stenosis. The narrowing begins at the sinotubular junction (arrows) and is associated with increased echogenicity of the vessel walls. (Courtesy of T. R. Kimball, MD, and S. A. Witt, RDCS.) |
False-positive results are even less common. Occasionally, a mild increase (1.5-2 m/sec) in descending aortic flow velocity will be misinterpreted as evidence of coarctation. In the absence of turbulence or echocardiographic evidence of vessel narrowing, this should generally be attributed to normal acceleration around the arch. Long-term follow-up after repair of aortic coarctation relies heavily on echocardiographic methods for the detection of restenosis. Estimation of the restenosis gradient by Doppler imaging is possible and correlates well with catheterization-derived values (Fig. 20.41).
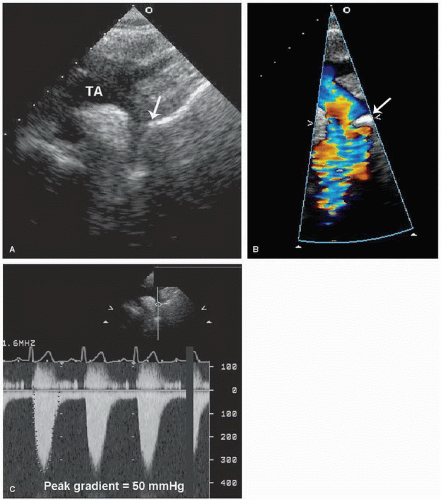 FIGURE 20.37. Coarctation of the aorta is evaluated from the suprasternal window. A: A long-axis view of the aortic arch suggests tapering of the descending aorta just beyond the origin of the left subclavian artery (arrow). B: Color flow imaging is useful to confirm turbulence and acceleration of flow at the level of the coarct (arrow). C: Then, continuous wave Doppler imaging is used to quantify the pressure gradient. In this case, a peak systolic gradient of 50 mm Hg was recorded. TA, transverse aorta. |
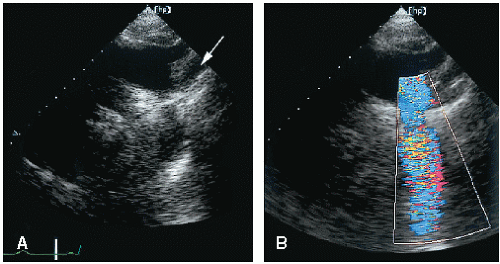 FIGURE 20.38. A: The location of the coarctation relative to the branch arteries. The left subclavian artery (arrow) is seen proximal to the site of obstruction. B: Color Doppler imaging demonstrates turbulence at the site of the coarctation. |
it is usually best seen from the suprasternal window. A patent ductus arteriosus (usually large) will also be present. When aortic arch interruption is suspected, a careful search for a right aortic arch should be undertaken to avoid confusion between these two entities.
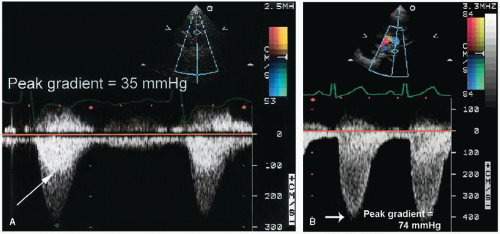 FIGURE 20.39. A: Continuous wave Doppler imaging demonstrates a peak systolic pressure gradient of 35 mm Hg across the coarctation. Superimposed within the systolic flow signal is a darker jet (arrow) that corresponds to flow proximal to the stenosis. Note the absence of flow during diastole. B: A more severe case of coarctation, with a peak gradient of 74 mm Hg. Note the persistence of low velocity flow throughout diastole. |
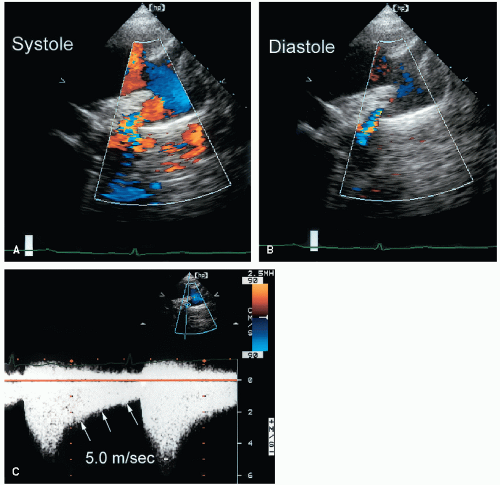 FIGURE 20.40. A case of severe coarctation of the aorta. Color Doppler images during systole (A) and diastole (B) demonstrate a high-velocity turbulent jet at the level of obstruction. The persistence of the jet throughout diastole is an indicator of its severity. C: Continuous wave Doppler imaging demonstrates a peak gradient of approximately 100 mm Hg. Note the persistence of the gradient throughout diastole (arrows).
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|