 imaging is a technique that allows for the determination of iron deposition in the myocardium, useful in disease states such as thalassemia and sickle cell disease to monitor and alter chelation therapy.
imaging is a technique that allows for the determination of iron deposition in the myocardium, useful in disease states such as thalassemia and sickle cell disease to monitor and alter chelation therapy.Table 73.1 CMR—Advantages and Limitations | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
and a lower amplitude signal from tissue and is usually utilized for cardiac motion, calculation of cardiac index, blood flow, and functional analysis (ventricular volumes, ejection fraction, etc.). One of the distinct advantages CMR has is that it does not rely on geometric assumptions to calculate volume, mass, and so on as other imaging modalities do. 3D echocardiography has come a long way, however, is not ubiquitous and needs specialized hardware, software, and image acquisition; CMR is nevertheless considered the “gold standard” in ventricular volume and mass measurement. Nearly all manuscripts in the literature validating 3D echocardiography compares the data with CMR; why use a surrogate, however, when a “gold standard” can be used? This is extremely important in CHD where bizarre, misshapen cardiovascular structures cannot be modeled by geometry. Further, CMR is exquisitely sensitive to turbulence and can detect even small amounts of regurgitation or stenosis. If turbulent blood flow is present, cine CMR will show a signal void in the region of turbulence, used to detect valvular regurgitation, valve stenosis, blood vessel stenosis, or baffle leaks/fenestrations (Figs. 73.1 and 73.4). Alternatively, cine CMR can obtain static images at various levels of the body, “labeling” blood as signal intense regions. This may be used, for example, to find collateral vessels off the aorta in a patient with tetralogy of Fallot and pulmonary atresia. Cine CMR can be of the spoiled gradient echo type (SGE) or of the SSFP type.
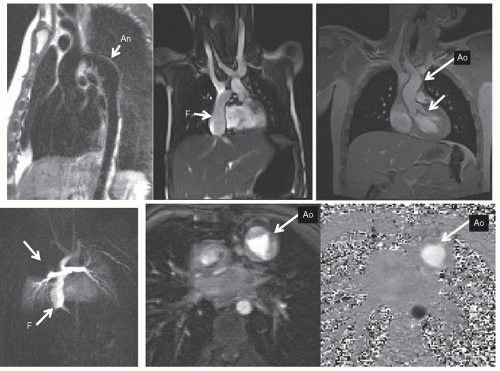 Fig. 73.1. Types of cardiac magnetic resonance in common use for anatomy. The upper left panel is a double-inversion dark blood image of a patient with a coarctation of the aorta (Ao) with residual aneurysm (An). Note that the blood is “black” and myocardial and vascular tissue give off signal. The upper middle image is a steady-state free precession (SSFP) image of a patient with pulmonary atresia with intact ventricular septum after Fontan (F); note how bright the blood is compared with the rest of the anatomy. SSFP depends upon this signal contrast for quality imaging. The upper right image is a patient with bicuspid aortic valve and mild aortic insufficiency using a spoiled gradient echo (SGE) sequence; note the turbulence underneath the aortic valve from the narrow jet. The lower left image is a three-dimensional maximum intensity projection of the Fontan baffle in a patient with hypoplastic left heart syndrome outlining the baffle, the branch pulmonary arteries and lungs; note the perfusion defect in the right upper lobe (arrow). The lower middle image is a magnitude image from phase-contrast velocity mapping depicting the trileaflet aortic valve in the Fontan patient mentioned in this figure; note how easily the valve leaflets are seen. The lower right image is the phase image in through plane-phase contrast velocity mapping of the aortic valve in the Fontan patient mentioned in this figure; flow, not just velocity, can be measured from this type of imaging. |
CMR, velocity can be encoded in “through plane”—that is into and out of the plane of the image—the result being that actual flow can be obtained. If a blood vessel is imaged in cross section, all the voxels that encode velocity in the vessel can be summed over the entire cross section of the vessel and integrated over the entire cardiac cycle to obtain flow (as in liters/minute, not just velocity). This can be done in nearly any vessel in the body—arterial or venous. Qp/Qs (Fig. 73.6), aortic to pulmonary collateral flow, regional flow to each lung, caval return can all be measured. CMR has the further advantage of performing internal checks—such as flow in the main pulmonary artery equaling the sum of the flows in the branch pulmonary arteries or the flow in the aorta equaling the sum of caval return in the absence of aortic to pulmonary collaterals; this is unique to CMR as a noninvasive imaging modality. Generally, an upper limit to the velocity to be measured is set, similar to the Nyquist limit in echocardiography, called the VENC (Velocity EN Coding). Also similar to echocardiography, velocity direction can be encoded in grayscale or color scale with “white” in one direction and “black” in another (or red and blue). Similar to Doppler echocardiography, velocity can also be encoded in the plane of the image—called “in-plane” velocity mapping. This can be encoded in either x– or y-directions of the image. The resulting three orthogonal planes that velocity can be measured in enable CMR to measure four-dimensional (4D) velocities when a “slab” is obtained, which encodes all three velocity vectors (three dimensions of velocity and one of time; Fig. 73.7). Much work is now being done in this area. Finally, phase-contrast CMR can be used to determine myocardial velocities similar to Doppler tissue imaging.
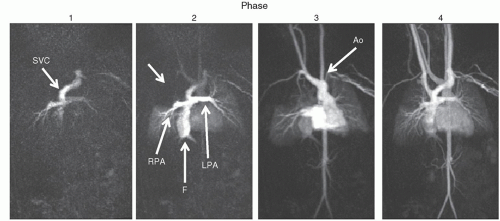 Fig. 73.2. Types of cardiac magnetic resonance in common use for anatomy—dynamic three-dimensional gadolinium imaging: The series of images, progressing from left to right, depicts the injection of gadolinium as it traverses the cardiovascular system in a patient with hypoplastic left heart syndrome after Fontan (F). Each phase is a 3D image in itself. In the left image, gadolinium is injected in the left arm and enters the superior vena cava (SVC) and the branch pulmonary arteries. In the image second to left, the gadolinium has lit up the F as well as the right (RPA) and left pulmonary arteries (LPA); note the perfusion defect in the right upper lobe (arrow). In the second image from the right, the left-sided phase of the injection depicts the aorta (Ao) and in the image on the right, the recirculation phase is seen with flow back into the RPA and LPA. |
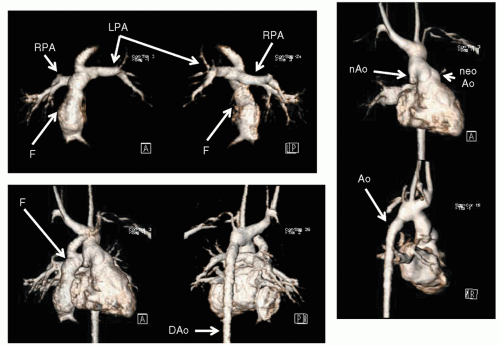 Fig. 73.3. Types of CMR in common use for anatomy—volume-rendered three-dimensional imaging: These volume-rendered images are from the patient in Figure 73.2. The advantage of dynamic 3D gadolinium imaging is that various phases can be separated out to highlight various structures. The upper left and middle panels are 3D volume renderings of the Fontan baffle (F) and right (RPA) and left pulmonary arteries (LPA) from anterior (left) and posterior (middle) views. The right upper and right lower panels are volume renderings of the ventricle and aorta (Ao) from the systemic phase of the dynamic 3D gadolinium injection; note how both the native (nAo) and neoaortas (neoAo) and the connections can be easily seen. The lower middle and lower left panels are a combination of the pulmonary and systemic phases demonstrating the entire heart intact. DAo, descending aorta. |
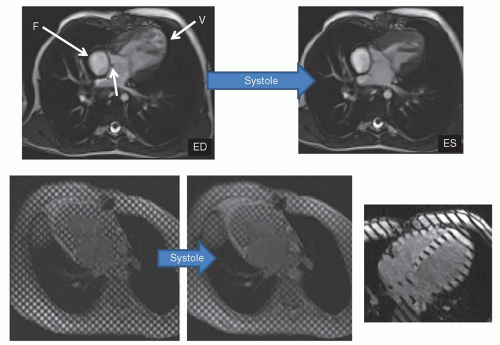 Fig. 73.4. Types of cardiac magnetic resonance in common use for physiology/function—cine CMR and myocardial tagging: The upper left and right panels are two images from the “three-chamber” cine of a patient with hypoplastic left heart syndrome after Fontan at end diastole (ED) and end systole (ES), respectively. Temporal resolution can be 20 milliseconds or less. The lower left and middle images are myocardial tagging (SPAMM—SPAtial Modulation of Magnetization) imaging of a single-ventricle patient at ED and ES; note how one can visualize the myocardial deformation of each “cube” of myocardium. Myocardial wall motion and three-dimensional strain can be measured. The right lower image is also myocardial tagging but of the one-dimensional version, used to tag thin walls such at the right ventricle in this four-chamber view; regional myocardial wall shortening fractions can be measured. |
as anomalous left coronary artery from the pulmonary artery or anomalous coronary artery origins from the opposite sinus, (2) acquired coronary artery abnormalities such as Kawasaki’s disease, and (3) iatrogenic coronary artery abnormalities such as those associated with repair of transposition of the great arteries or the Ross procedure. CMR generally utilizes 3D, fat saturated (to suppress the signal from epicardial fat), T2 prepared (to suppress signal from myocardial muscle) sequences along with navigator techniques (a CMR technique that monitors diaphragmatic motion) to allow for coronary imaging in even small infants (Fig. 73.9).
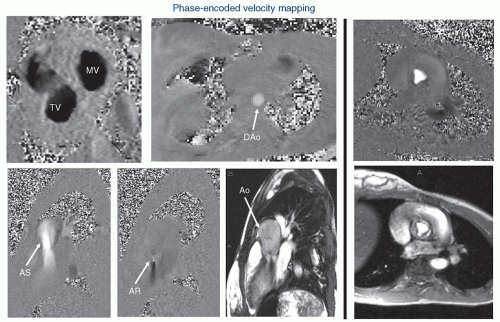 Fig. 73.5. Types of cardiac magnetic resonance in common use for physiology/function—velocity mapping: Each pixel has a velocity measurement associated with it and encodes velocity into and out of the plane of the image for the through-plane version and in the plane for the in-plane version. Direction is encoded as either increased signal (white) in one direction and decreased signal (black) in the other direction. Summation of the multiplication of pixel areas by their respective velocities yields flow in the through-plane version. Through-plane velocity mapping—the upper left image is a velocity map across the atrioventricular valves in a patient with transposition of the great arteries, whereas the upper middle panel is an axial phase-encoded velocity map of the descending aorta (DAo). The upper right and lower right panels demonstrate the velocity map and anatomic image, respectively, across a normal trileaflet aortic valve. In-plane velocity mapping—the lower left and second from left images are in-plane velocity maps and the anatomic image (third from left) of the left ventricular outflow tract of a patient with aortic stenosis and insufficiency. The lower left image is in systole, the second and third from left in diastole. |
pulse; this ability of CMR to detect myocardial scar is unique in noninvasive imaging. Signal intensity differences between normal and infarcted myocardium of up to 500% have been achieved. The technique has been shown to accurately delineate the presence, extent, and location of acute and chronic myocardial infarction as well as fibrous tissue (Fig. 73.10). Ventricular septal defect patches, right ventricular outflow tract patches as with repaired tetralogy of Fallot also demonstrate signal intensity with this technique. In addition, various cardiac tumors can take up gadolinium, whereas others will not and cardiac MR uses this property, along with T1-weighted images, T2-weighted images, and fat saturation to predict what type of tumor is present (Fig. 73.11).
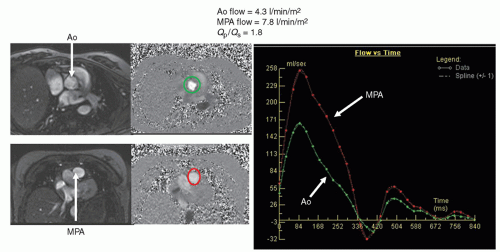 Fig. 73.6. Types of cardiac magnetic resonance in common use for physiology/function—velocity mapping analysis example—Qp/Qs: velocity mapping can determine complex or simple flows. For example, in a patient with an atrial or ventricular septal defect, Qp/Qs may be determined by placing a velocity map across the aortic (Ao) valve (top left and top middle panels) and the main pulmonary artery (MPA) (lower left and lower middle panels). The left panels are the anatomic images for reference, and the middle panels are the velocity maps with the cross section of the vessel contoured (green for Ao and red for MPA). The resultant measurements are graphed in a flow versus time curve (right panel). In this particular patient with partial anomalous pulmonary venous connection, Qp/Qs was 1.8. |
X-ray magnetic resonance (XMR)—the use of CMR in combination with cardiac catheterization. The uses range from superimposition of 3D images generated by CMR onto the fluoroscopy of the catheterization laboratory to act as a “roadmap” for the physician performing the catheterization to performing interventions in the CMR suite—and everything in-between.
Computational fluid dynamic modeling is the application of the Navier-Stokes equations, which is the governing equations of fluid flow in the body, to the cardiovascular system. With anatomy from CMR and blood flow measured at the inlets and outlets of the system (e.g., cavae and branch pulmonary arteries of the systemic venous pathway of Fontan patients or the main and branch pulmonary arteries in tetralogy of Fallot), a model of fluid flow can be created and tested at different flow conditions.
Exercise CMR—Performing exercise in the CMR suite itself with a CMR-compatible ergometer. Ventricular function, blood flow, and perfusion at exercise can be obtained by utilizing “real time” cine CMR and “real time” phase-contrast velocity mapping (Fig. 73.12).
Fetal CMR—Utilizing “real time” and ultrafast single shot CMR, fetal cardiac anatomy and ventricular function can be obtained. Newer techniques utilize “Metric Optimized Gating” (MOG) allow for measuring flow in fetal vessels (Fig. 73.12).
Tissue characterization: BOLD imaging, still being developed, can measure tissue oxygen levels as deoxygenated blood
has different magnetic properties than oxygenated blood. T1 mapping utilizing gadolinium can measure “diffuse” myocardial scarring.
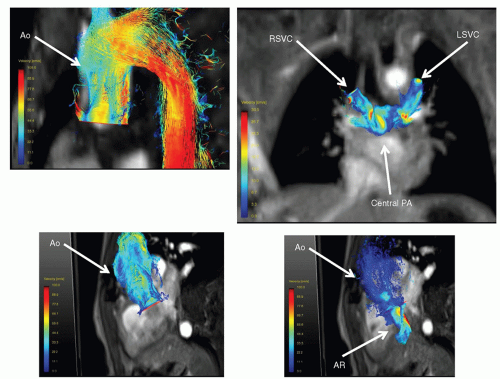
Fig. 73.7. Types of cardiac magnetic resonance in common use for physiology/function— four-dimensional (4D) velocity mapping: By obtaining a “slab” encoding all three velocity vectors, 4D flows can be visualized by streamlines. The upper left panel is 4D flow in the aorta (Ao) of a patient with transposition of the great arteries after arterial switch operation. Lower left and right panels are 4D flows of a patient with a bicuspid Ao valve and aortic insufficiency (AR) with frames in systole (left) and diastole (right), the plane which the streamlines originating from being the aortic annulus. The upper right image demonstrates 4D flows in a patient with single ventricle after bilateral, bidirectional Glenn. Central PA, central PA; LSVC, left superior vena cava; RSVC, right superior vena cava.
Three-dimensional printing is a technique that enables creation of physical 3D models of the cardiovascular system from gadolinium images, which the surgeon or the cardiologist can actually hold in their hands (Fig. 73.12).
T1 mapping: The new and emerging field of “diffuse” myocardial scarring has been developing for a few years. As opposed to viability imaging, which generally detects discreet areas of scar, T1 mapping techniques utilizes gadolinium to detect diffuse scarring not readily apparent on the viability images.
For example, if a coarctation of the aorta or the systemic venous pathway of a Fontan patient is being imaged, an off-axis sagittal image is used to obtain the “candycane” view of the aorta or the long axis of the systemic venous pathway (parallel to the path of flowing blood). If on the other hand, a double aortic arch is being imaged or the left ventricular outflow tract is assessed, a set of straight or slightly off-axis coronal images are obtained to yield the short axes of the right and left aortic arches, the long axes of the amalgamation of these structures into ascending and descending aorta, and the long axis of the left ventricular outflow tract. This can be performed using either dark or bright blood techniques.
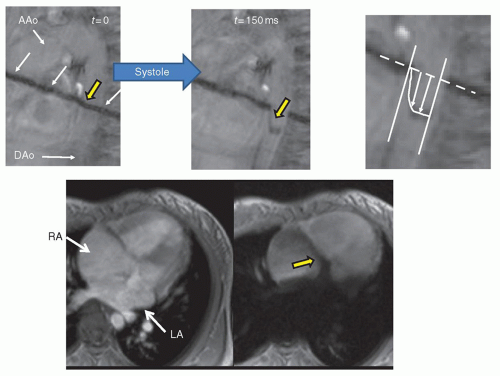 Fig. 73.8. Types of cardiac magnetic resonance in common use for physiology/function—blood tagging: Upper left and upper middle panels display blood (Bolus) tagging in the descending aorta (DAo) in the candy-cane view at end-diastole (t = 0) and 150 milliseconds into systole (t = 150 ms). White arrows represent the site of initial tagging and the yellow arrow is the tag in the DAo. Note the velocity profile of the DAo in the upper middle panel. The upper right panel is a magnification of the site of tagging in the DAo, showing how velocities at each point across the vessel diameter are measured. With the appropriate mathematical calculation, planimeterizing of the area underneath the velocity profile will yield the regional cardiac index; this technique for calculating cardiac index has been supplanted by phase-encoded velocity mapping. The lower two images demonstrate blood tagging of the left atrium (LA) and ventricle in a patient with a primum atrial septal defect. The left lower panel is the cine image without tagging the left side of the heart and the right image is one with the tag (large black line across the left side of the heart). The yellow arrow points to flow across the primum defect from LA to right atrium (RA). AAo, ascending aorta. |
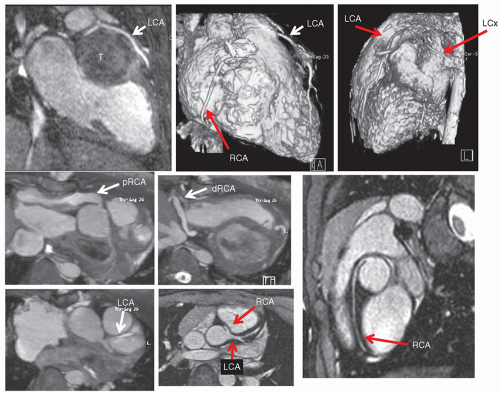 Fig. 73.9. Types of cardiac magnetic resonance (CMR) in common use—coronary imaging: CMR has come into to its own with whole heart, steady-state free precession (SSFP) imaging for coronaries that have compared favorably to catheter and CT (although resolution is less). The upper three images are of a patient with a left ventricular fibroma. The top left panel is an SSFP image of the left coronary artery (LCA)—specifically the left anterior descending coronary artery—coursing just above the tumor. The middle and right panels are 3D reconstructions demonstrating the courses of the right coronary artery (RCA), LCA and the left circumflex coronary artery (LCx); because the tumor is nearly avascular, it is not imaged on the 3D reconstruction. The middle left, second from middle and the lower left panels are taken from a patient who is after heart transplantations with large coronary aneurysms of both the right and left systems. The lower middle panel and lower right panel are from a patient with anomalous origin of the RCA from the left coronary cusp. |
disease and history. Myocardial tagging or blood tagging can be done after the cine sequences. Coronary imaging can take anywhere from 7 to 10 minutes and if that was the goal, it would be performed after the initial static images and some cine imaging. If perfusion is the goal of the study, this is usually done close to the beginning of the exam but after all dark blood sequences are needed. If myocardial iron imaging (
 imaging) was the goal, that would be performed first. In the case of perfusion, the following sequence of events would be used, taking 60 to 70 minutes:
imaging) was the goal, that would be performed first. In the case of perfusion, the following sequence of events would be used, taking 60 to 70 minutes: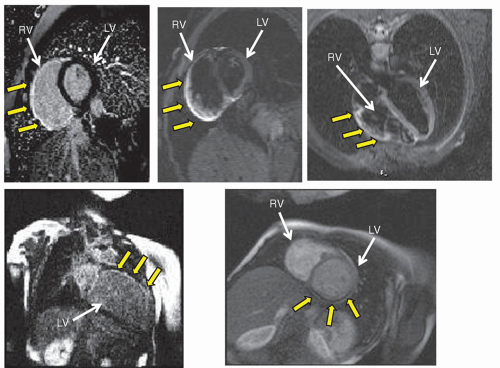 Fig. 73.10. Types of cardiac magnetic resonance in common use for tissue characterization—viability, edema imaging (T2), and perfusion: delayed enhancement imaging, also known as viability, can detect scar/fibrous tissue; surgically implanted foreign material such as a patch; or can aid in tumor characterization. The infarcted tissue is signal intense (white) while normal myocardium is black (see text). The upper and lower left panels display a patient with right ventricular (RV) infarction in short axis (yellow arrows) and superior wall endocardial scarring of the left ventricle in long axis (yellow arrows), respectively. Normal myocardium should appear black as the left ventricle (LV) in the upper left image. The patient with an RV infarction also demonstrated myocardial edema (yellow arrows) with T2 imaging in the upper middle (RV short axis) and upper right panels (the four-chamber view). Perfusion imaging uses gadolinium injection, and visualization of the myocardial “blush” indicates the degree of myocardial perfusion. The lower right panel is a perfusion image of a patient with transposition of the great arteries after arterial switch operation. Note the inferior and lateral wall perfusion defect of the LV (yellow arrows) with adenosine administration. |
Static bright blood imaging
Cine imaging to obtain a gestalt for myocardial shortening prior to adenosine
Adenosine perfusion imaging with gadolinium (adenosine 140 µg/kg/minutes for 4 to 6 minutes)
Cine imaging for function (ventricular volumes and mass)
Velocity mapping for flows
Resting perfusion imaging with gadolinium (15 to 20 minutes after adenosine perfusion)
Coronary imaging
Delayed enhancement
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


