The aortic valve is a complex, intricate structure with remarkable durability. It is composed of three cusps of equal size, each of which is surrounded by a sinus. The cusps are separated by three commissures and supported by a fibrous annulus. Each cusp is crescent shaped and capable of opening fully to allow unimpeded forward flow, then closing tightly to prevent regurgitation. The free edge of each cusp curves upward from the commissure and forms a slight thickening at the tip or midpoint, called the node of Arantius. When the valve closes, the three nodes meet in the center, allowing coaptation to occur along three lines that radiate out from this center point. Overlap of valve tissue along the lines of closure produces a tight seal and prevents backflow during diastole. When viewed from a conventional echocardiographic short-axis projection, these three lines of closure are recorded as a Y shape.
Behind each cusp is its associated sinus of Valsalva. The sinuses represent outpouchings in the aortic root directly behind each cusp. They function to support the cusps during systole and provide a reservoir of blood to augment coronary artery flow during diastole. The sinus and its corresponding cusp share the same name. The left and right coronary arteries arise from the left and right sinuses, respectively, and are associated with the left and right aortic cusps. The third, or noncoronary sinus, is posterior and rightward, just above the base of the interatrial septum, and is associated with the noncoronary aortic cusp. At the superior margin of the sinuses, the aortic root narrows at the sinotubular junction.
Diseases of the aortic valve may be either congenital or acquired and may produce either stenosis or regurgitation or a combination of the two. The most common causes of acquired aortic valve disease in adults are degenerative, rheumatic, and infective. Diseases of the aorta may also affect aortic valve function. Subaortic obstruction may also occur. This is due to either hypertrophic cardiomyopathy (see Chapter 19) or membranous and fibromuscular subaortic stenosis (see Chapter 20).
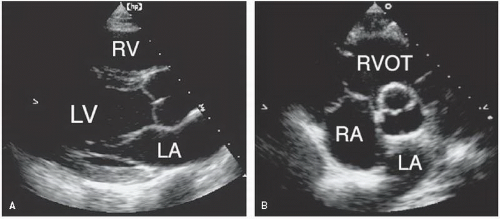
FIGURE 11.1. A functionally normal bicuspid aortic valve from a young patient. A: The long-axis view demonstrates doming of the valve in systole. B: The basal short-axis view confirms that the valve is bicuspid but with no evidence of stenosis.
Aortic Stenosis
Although obstruction to left ventricular outflow can occur at multiple levels, valvular aortic stenosis is most common. Congenitally abnormal valves may be stenotic at birth or may develop both stenosis and regurgitation over time. Typically, such valves are bicuspid, usually the result of fusion of the right and left coronary cusps. They demonstrate systolic “doming” and tend to become functionally abnormal during adolescence or early adulthood (Figs. 11.1 and 11.2). This form of aortic valve disease is covered more fully in Chapter 20. Many cases of aortic stenosis are acquired, that is, the valves are normal at birth but become gradually dysfunctional over time. The goals of the echocardiographic evaluation of this condition include establishing a diagnosis, quantifying severity, and assessing left ventricular function. A summary of the indications for echocardiography in the setting of valvular stenosis is provided in Table 11.1.
Appropriateness criteria have also been published to offer guidance in the proper application of echocardiography to patients with known or suspected aortic stenosis (Table 11.2). Echocardiography is considered “appropriate” when used for the initial evaluation of known or suspected aortic stenosis, for the routine annual evaluation of asymptomatic severe aortic stenosis, and for the reevaluation of aortic stenosis if there is a change in clinical status. It is considered inappropriate to perform echocardiography for the routine annual reevaluation of asymptomatic mild aortic stenosis, unless there is a change in clinical status.
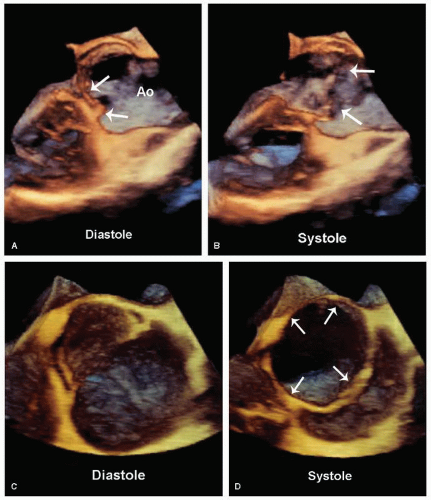
FIGURE 11.2. A three-dimensional transesophageal echocardiogram of a bicuspid aortic valve, recorded in systole (panels B and D) and diastole (panels A and C). Three-dimensional imaging provides a unique perspective, demonstrating doming of the valve in the long axis (panel B, arrows) and fusion of cusps in the short axis (panel C).
Table 11.1 Indications for Echocardiography in Valvular Stenosis
Indication
Class
1.
Diagnosis; assessment of hemodynamic severity
I
2.
Assessment of left and right ventricular size, function, and/or hemodynamics
I
3.
Reevaluation of patients with known valvular stenosis with changing symptoms or signs
I
4.
Assessment of changes in hemodynamic severity and ventricular compensation in patients with known valvular stenosis during pregnancy
I
5.
Reevaluation of asymptomatic patients with severe stenosis
I
6.
Assessment of the hemodynamic significance of mild to moderate valvular stenosis by stress Doppler echocardiography
IIa
7.
Reevaluation of patients with mild to moderate aortic stenosis with left ventricular dysfunction hypertrophy even without clinical symptoms
IIa
8.
Reevaluation of patients with mild to moderate aortic valvular stenosis with stable signs and symptoms
IIb
9.
Dobutamine echocardiography for the evaluation of patients with low-gradient aortic stenosis and ventricular dysfunction
IIb
10.
Routine reevaluation of asymptomatic adult patients with mild aortic stenosis having stable physical signs and normal left ventricular size and function
III
Adapted from Cheitlin MD, Alpert JS, Armstrong WF, et al. ACC/AHA Guidelines for the Clinical Application of Echocardiography: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Clinical Application of Echocardiography). Developed in collaboration with the American Society of Echocardiography. Circulation 1997;95:1686-1744, with permission, and Bonow RO, Carabello BA, Chatterjee K, et al. 2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on management of patients with valvular heart disease. J Am Coll Cardiol 2008;52:e1-e142.
Table 11.2 Appropriateness Criteria for Aortic Valve Disease
Indication
Appropriateness Score (1{9)
Criteria
Murmur
17.
Initial evaluation of murmur in patients for whom there is a reasonable suspicion of valvular or structural heart disease
A (9)
Native Valvular Stenosis
20.
Initial evaluation of known or suspected native valvular stenosis
A (9)
22.
Routine (yearly) evaluation of an asymptomatic patient with severe native valvular stenosis
A (7)
23.
Reevaluation of a patient with native valvular stenosis who has had a change in clinical status
A (9)
21.
Routine (yearly) reevaluation of an asymptomatic patient with mild aortic stenosis and no change in clinical status
I (2)
Native Valvular Regurgitation
24.
Initial evaluation of known or suspected native valvular regurgitation
A (9)
26.
Routine (yearly) reevaluation of an asymptomatic patient with sever native valvular regurgitation with no change in clinical status
A (8)
27.
Reevaluation of native valvular regurgitation in patients with a change in clinical status
A (9)
25.
Routine (yearly) reevaluation of native valvular regurgitation in an asymptomatic patient with mild regurgitation, no change in clinical status, and normal LV size
I (2)
LV, left ventricle.
Reprinted with permission of the ACCF from Douglas PS, Khandheria B, Stainback RF, et al. ACCF/ASE/ACEP/ASNC/SCAI/SCCT/SCMR 2007 appropriateness criteria for transthoracic and transesophageal echocardiography. J Am Coll Cardiol 2007;50(2):187-204.
These are reasonable recommendations based on available evidence, known natural history data, and expert consensus panel opinion. They underscore several important factors including (1) the proper timing of reevaluation, (2) the expected rate of progression of disease, and (3) the importance of symptoms in patient management. Appropriate criteria cannot provide guidance for all possible clinical scenarios and individual judgment must be used to manage patients. Current criteria do not, for example, take into account the important confounding effects of left ventricular dysfunction or coexisting coronary disease.
The simultaneous assessment of left ventricular function is important because of its prognostic and management implications. In addition, reduced left ventricular function alters the relationship between transvalvular pressure gradient and aortic valve area, thereby complicating the quantitative determination of severity. Other related factors that must be evaluated include the presence and extent of proximal aorta dilation, coexisting mitral valve disease, a measurement of pulmonary artery pressure, and coexisting coronary artery disease.
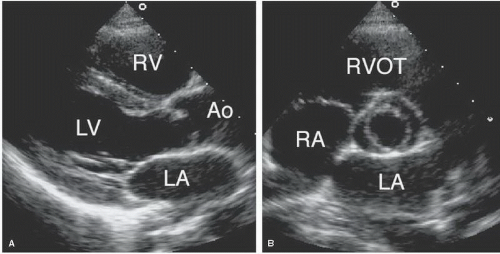
FIGURE 11.3. A normal aortic valve. Both images were recorded during diastole. A: The long-axis view demonstrates the appearance of a typical normal aortic valve in the closed position. B: The same valve is demonstrated from the short-axis view. Note that, because of shadowing and lateral resolution, the coaptation line between the left and noncoronary cusps is not visualized.
The qualitative diagnosis of aortic stenosis relies heavily on two-dimensional echocardiography. By observing the opening and closing of the valve in systole and diastole, respectively, the presence or absence of valvular stenosis can be determined with confidence. In normal subjects, the aortic valve cusps appear thin and delicate and may be difficult to visualize (Fig. 11.3). In the long-axis view, the cusps open rapidly in systole and appear as linear parallel lines close to the walls of the aorta (Fig. 11.4). With the onset of diastole, they come together and are recorded as a faint linear density within the plane of the aortic annulus. Because the velocity of valve motion during opening and closing is high relative to the frame rate of most echocardiographic systems, the normal aortic valve is usually visualized either fully opened or closed but rarely in any intermediate position. In the basal short-axis view, the three aortic cusps can be visualized within the annulus during diastole (Fig. 11.5). The three lines of coaptation can be recorded, normally forming a Y (sometimes referred to as an inverted Mercedes-Benz sign). With the onset of systole, the cusps open out of the imaging plane, providing a view of the aortic annulus. The short-axis perspective is most helpful to determine the number of cusps and whether fusion of one or more commissures is present. In patients who are difficult to image, normal leaflets are so delicate that they are hard to visualize, generally an indication that they are morphologically normal.
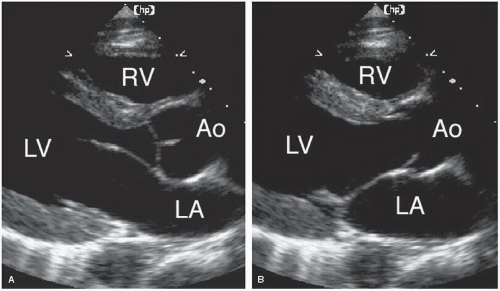
FIGURE 11.4. A normal aortic valve is shown during diastole in the closed position (A) and during systole in the open position (B).
With acquired valvular aortic stenosis, the cusps become thickened and restricted (Fig. 11.6). Their position during systole is no longer parallel to the aortic walls, and the edges are often seen to point toward the center of the aorta. In severe cases, a nearly total lack of mobility may be present and the anatomy may become so distorted that identification of the individual cusps is impossible. Unfortunately, attempts to quantify the degree of stenosis based on two-dimensional echocardiographic findings have been unsuccessful. However, useful qualitative information is almost always present. For example, thickened, calcified cusps that display preserved mobility define aortic sclerosis (typically associated with a peak Doppler velocity of ≤2.5 m/sec). Conversely, heavily calcified cusps with little or no mobility suggest severe stenosis. If one cusp is seen to move normally, critical aortic stenosis has been excluded. Figure 11.7 is an example of mild aortic stenosis. Although the diagnosis of aortic stenosis is apparent by two-dimensional imaging, the degree of severity can only be estimated. In the example, the cusps are thickened and exhibit restricted mobility. However, Doppler examination revealed only mild stenosis with a maximal pressure gradient of approximately 28 mm Hg. In this example, based solely on two-dimensional appearance, overestimation of severity would be likely. Figure 11.8 is of a patient with heart failure and moderate left ventricular dysfunction. Also note that the aortic valve is severely calcified with markedly restricted systolic mobility.
One approach to quantitation relies on transesophageal echocardiography. This technique is excellent for determining the morphology of abnormal aortic valves. From a shortaxis view at the level of the valve orifice, direct planimetry of the valve area is possible in more than 90% of patients (Fig. 11.9). Limitations of this approach include the irregular, three-dimensional nature of the orifice and the shadowing effect of a calcified valve and root. As a result, the technical challenges of this approach are considerable and it is not routinely performed.
Three-dimensional echocardiography may provide some advantages in this regard, specifically by offering more accurate visualization of the stenotic orifice (Fig. 11.10). Several studies have now confirmed the feasibility of this approach. However, the shadowing effect of calcified cusps remains a limitation. In addition, the challenges of precise planimetry of a very small area, where even small absolute errors may be significant, must be taken into account.
Doppler Assessment of Aortic Stenosis
The Doppler assessment of aortic stenosis begins with the determination of the maximal jet velocity through the stenotic valve. From this value, the simplified Bernoulli equation is used to estimate the peak instantaneous gradient. This approach has been validated both in in vitro and in clinical situations. It has proved to be a practical, noninvasive method for determining the pressure gradient across the aortic valve, correlating well with simultaneous measurements obtained by invasive means.
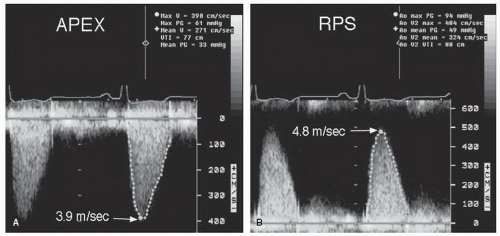
An accurate Doppler assessment of aortic stenosis depends on one’s ability to record the maximal jet velocity through the stenotic orifice (Fig. 11.11). As blood accelerates through the valve, peak velocity coincides temporally with the maximal pressure gradient. Peak velocity usually occurs in midsystole. As aortic stenosis worsens, velocity tends to peak later in systole and the shape becomes more rounded and less peaked. Late-peaking jets are also characteristic of dynamic subaortic stenosis, as occurs in hypertrophic cardiomyopathy (Fig. 11.12). Multiple windows, including the apical five-chamber, suprasternal, and right parasternal, should be used in an attempt to align the Doppler beam with the direction of flow of the stenotic jet. Failure to achieve parallel alignment will result in underestimation of true velocity (Fig. 11.13). Both imaging and nonimaging continuous wave transducers should be used. Because the direction of jet flow is difficult to predict from two-dimensional imaging, color Doppler imaging may be used to improve alignment. Careful manipulation of the transducer position to achieve optimal alignment is recommended. In practice, a thorough and patient interrogation using all available echocardiographic windows is undertaken to record the highest velocity signal possible. The highest jet velocity obtained, regardless of location, should then be used for calculation of the gradient. By carefully adjusting patient position and instrument gain, both the full envelope and the peak velocity of the stenotic jet can be obtained. In Figure 11.13, the peak gradient would have been underestimated if the echocardiographer had concluded the examination with the apical views rather than moving to the right parasternal window where a higher velocity was recorded.
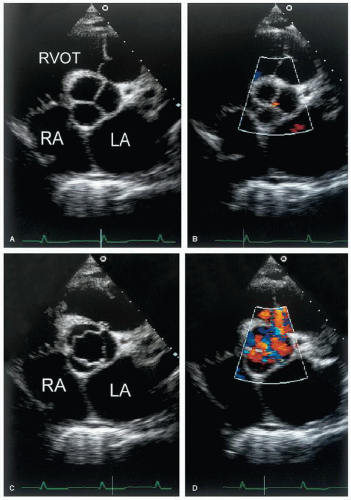
FIGURE 11.5. A normal tricuspid aortic valve is shown with and without color Doppler. A: The short-axis view demonstrates the three cusps during diastole. B: A diastolic frame with color flow imaging demonstrates trivial aortic regurgitation. C: The valve is shown during systole demonstrating the orifice in an open position. D: Color flow imaging during systole demonstrates the flow through the valve.
From the Doppler recording, the peak instantaneous and mean pressure gradient can be determined from the simplified Bernoulli equation (Fig. 11.14). The maximal gradient is derived from the equation:
where v equals the maximal jet velocity expressed in meters per second. This represents a significant simplification of the complete Bernoulli equation. For example, it assumes that the distal velocity is sufficiently greater than the proximal velocity that the latter can be ignored. However, in cases where the proximal velocity is greater than 1.5 m/sec and the distal velocity is only modestly elevated (less than 3.5 m/sec), the proximal velocity cannot be ignored and the more complete form of the equation should be used:
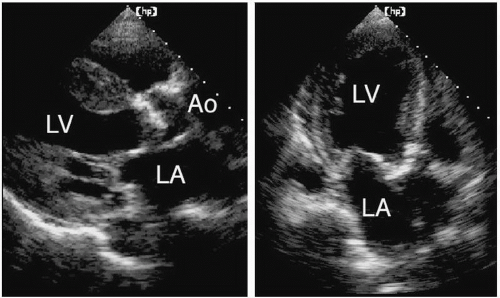
FIGURE 11.6. A two-dimensional echocardiogram from a patient with severe aortic stenosis. A: The long-axis view reveals an echogenic and very immobile aortic valve. B: The corresponding short-axis view suggests a high degree of calcification of the valve and minimal mobility during systole.
FIGURE 11.7. A patient with mild aortic stenosis. See text for details.
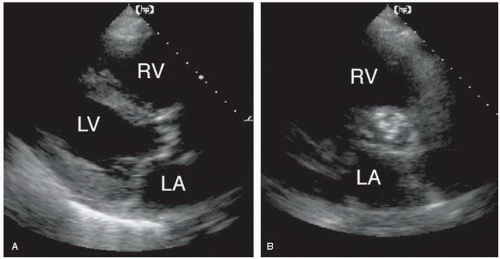
FIGURE 11.8. An example of severe aortic stenosis in the setting of left ventricular dysfunction. The valve is calcified and immobile. A qualitative diagnosis of aortic stenosis is possible, but no quantitative information is available.
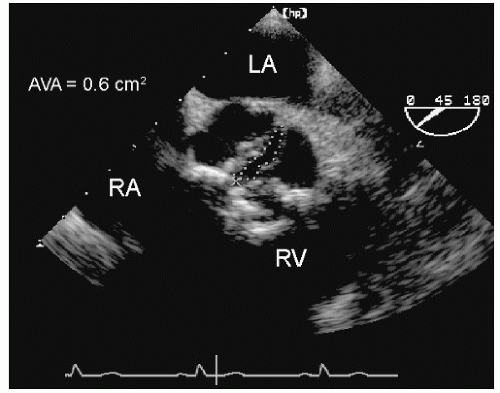
FIGURE 11.9. A transesophageal echocardiogram demonstrates the method of direct planimetry of the aortic valve orifice. By carefully adjusting the level of the short-axis plane, the orifice can be visualized in most patients. In this example, severe stenosis was confirmed. AVA, aortic valve area.
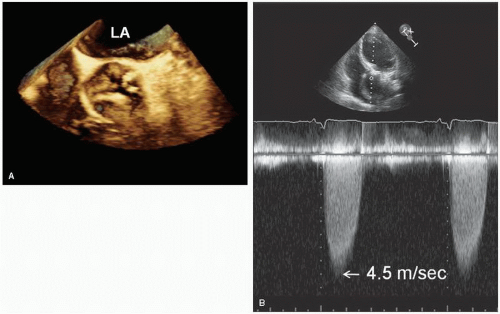
FIGURE 11.10. A volume-rendered three-dimensional transesophageal echocardiogram from a patient with degenerative aortic stenosis. In panel A, the valve is viewed from above with the ascending aorta cut away. The three cusps with greatly restricted mobility are visualized. This is an example severe aortic stenosis with a maximal gradient of 80 mm Hg (panel B).
Situations in which this is relevant include severe aortic regurgitation (due to high forward stroke volume) or when stenoses appear in series, such as combined valvular and subvalvular stenosis.
The mean pressure gradient is most often obtained by planimetry of the Doppler envelope, which allows the computer to integrate the instantaneous velocity data and provide a mean value. It should be emphasized that mean gradient cannot be obtained by squaring the mean velocity. Because of the nearly linear relationship between mean gradient and maximal gradient, the mean pressure gradient can also be estimated from the formula:
Stated differently, Equation 11.2 suggests that mean gradient is approximately two thirds of the peak instantaneous gradient. Both mean and peak gradients should be reported.
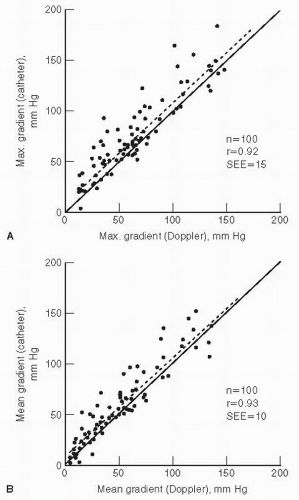
The accuracy of the Bernoulli equation to quantify aortic stenosis pressure gradients is well established (Fig. 11.15). Selective studies that have validated the modified Bernoulli equation against invasive hemodynamic measurements are shown in Table 11.3. As can be seen from Figure 11.15, Doppler gradients tend to be slightly higher than corresponding values obtained in the catheterization laboratory. Such differences are not due to the inaccuracy of either technique but most likely the result of pressure recovery, which is discussed in detail in Chapter 9. In the setting of native valve aortic stenosis, some recovery of pressure downstream from the vena contracta can be expected. This occurs as the jet expands and decelerates downstream from the vena contracta resulting in a lower net pressure gradient compared to peak pressure gradient. The net gradient is measured in the catheterization laboratory, typically as the difference in pressure between the left ventricle and ascending aorta. The peak pressure gradient is derived from continuous wave Doppler by measuring the highest velocity within the vena contracta at the level of the orifice. In most cases, pressure recovery has a negligible effect on the accuracy of gradient calculation. Situations in which pressure recovery may be more significant include small aortic root (e.g., less than 3.0 cm in diameter), domed congenital aortic stenosis, and with certain types of prosthetic valves. In such cases, Doppler will record a higher pressure gradient within the vena contracta, while the catheter-derived pressure will likely be obtained further downstream and will record a lower gradient. These methodological differences provide a plausible explanation for the slightly higher gradients derived by Doppler versus catheterization techniques.
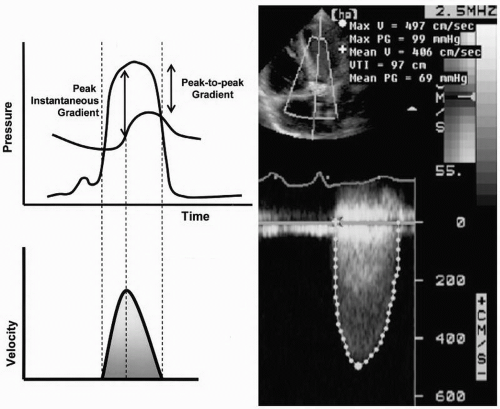
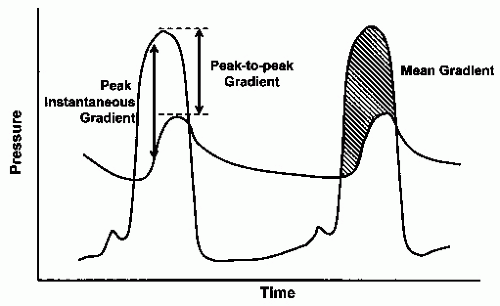
FIGURE 11.11. Left: The schematic demonstrates the relationship between the pressure gradient across a stenotic aortic valve and the velocity tracing obtained by Doppler. The differences between peak-to-peak and peak instantaneous gradients are illustrated. The maximal flow velocity obtained with Doppler imaging corresponds temporally with the peak instantaneous gradient. Right: A Doppler recording from a patient with severe aortic stenosis demonstrates a peak instantaneous gradient of approximately 100 mm Hg.
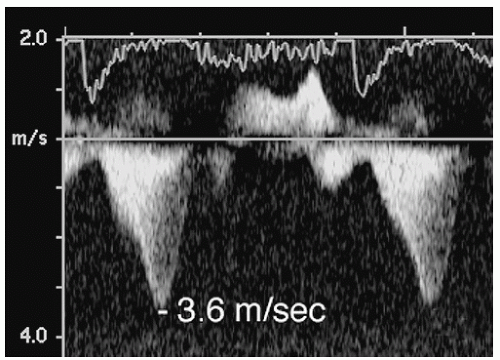
FIGURE 11.12. A late-peaking gradient from a patient with hypertrophic cardiomyopathy. This obstruction occurs at the level of the left ventricular outflow tract and results in a gradient of approximately 50 mm Hg. Note the contour of the jet with acceleration of flow in mid and late systole.
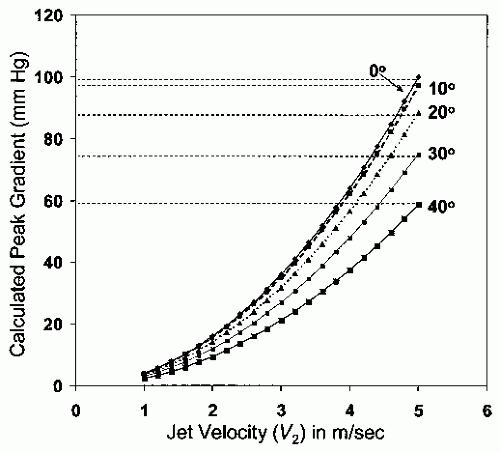
Despite the generally excellent agreement between Doppler and invasive methods, errors can occur. When discrepancies in measurements happen, several possibilities should be considered. First, the technical quality of the Doppler data should be examined. A technically poor recording may fail to display the highest velocity signals, resulting in underestimation of the true gradient. An inability to align the interrogation angle parallel to flow also results in underestimation. This relationship is demonstrated in Figure 11.16. The various curves plot the relationship between jet velocity and calculated peak gradient (using the Bernoulli equation), assuming different values for angle θ. Note that for low velocity jets (<3 m/sec), the magnitude of the error introduced by angle misalignment is relatively modest. For patients with severe aortic stenosis, errors in alignment cause substantial underestimation of true gradient. Also note that errors less than 20° result in a relatively insignificant degree of underestimation. However, as the intercept angle increases beyond 20°, the magnitude of error increases rapidly.
Because the Doppler technique measures velocity over time, Doppler-derived data always represent instantaneous gradients. It is customary in the cardiac catheterization laboratory to report the peak-to-peak gradient, which is often less than the peak instantaneous gradient. This is illustrated in Figure 11.14. It is well known that peak-to-peak gradients are contrived and never exist in time. Failure to recognize the differences in the reported data often leads to miscommunication of clinical information. This can be partially avoided through the use of mean gradients, which correlate better between catheterization and echocardiographic data. Finally, bear in mind that valve gradients are dynamic measurements that vary with heart rate, loading conditions, blood pressure, and inotropic state. Figure 11.17 is an example of varying jet velocities from a patient with an arrhythmia. Note how each recorded beat yields a different peak instantaneous gradient, ranging from approximately 35 to more than 100 mm Hg. If two tests are performed on different days, the results may be expected to vary. It is therefore not surprising that the best correlation between invasive hemodynamics and Doppler is achieved in studies in which the tests are performed simultaneously. When catheterization and Doppler results differ, both tests may be correct but may reflect variations in gradient over time.
FIGURE 11.13. Aortic stenosis should be quantified using Doppler from multiple windows. A: A recording from the apical view. B: A higher gradient is obtained from the right parasternal (RPS) window. See text for details.
Overestimation of the true pressure gradient is less common but can occur. This is usually the result of mistaken identity of the recorded signal. For example, the mitral regurgitation jet has a contour similar to that of a jet of severe aortic stenosis. Because of the similarities in location and direction of the two jets, mistaken identity can occur. To avoid this, the two jets should be recorded by sweeping the transducer back and forth to clearly indicate to the interpreter which jet is which. Another helpful clue involves the timing of the two jets (Fig. 11.18). Mitral regurgitation is longer in duration, beginning during isovolumic contraction and extending into isovolumic relaxation.
FIGURE 11.14. This schematic demonstrates the differences among peak-to-peak, peak instantaneous, and mean gradients. See text for details.
FIGURE 11.15. The correlation between Doppler and cardiac catheterization for measuring peak (A) and mean (B) gradients. The relationship is linear and a similar degree of correlation is shown for both mean and peak gradients. (From Currie PJ, Seward JB, Reeder GS, et al. Continuous-wave Doppler echocardiographic assessment of severity of calcific aortic stenosis: a simultaneous Doppler-catheter correlative study in 100 adult patients. Circulation 1985;71:1162-1169, with permission.)
Table 11.3 Correlation between Echocardiographic Doppler Techniques and Cardiac Catheterization for Assessing the Severity of Aortic Stenosis
c Echo-valve area by planimetry using transesophageal echocardiography.
SEE, standard error of the estimate.
FIGURE 11.16. The effect of incident angle (θ) on recorded velocity. When the angle is 0° (uppermost curve), the Bernoulli equation provides an accurate measure of gradient. As θ increases, an increasing degree of underestimation occurs. See text for details.
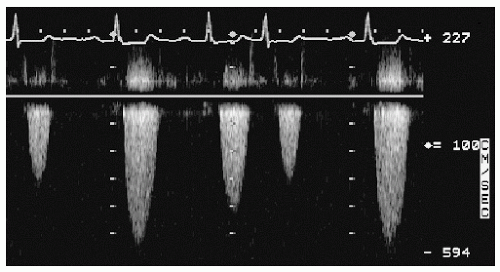
FIGURE 11.17. Doppler recording of aortic stenosis from a patient with an arrhythmia. Note the variability in velocity, depending on the stroke volume and the preceding R-R interval. See text for details.
FIGURE 11.18. The jets of aortic stenosis (AS) and mitral regurgitation (MR) can sometimes be confused. A helpful clue to differentiate between the two involves the timing of flow. A: Aortic flow begins after the period of isovolumic contraction. The vertical line provides a reference mark relative to the QRS of the electrocardiogram. Note the gap between the line and the onset of flow. B: The same line coincides with the onset of mitral regurgitation. This is because mitral regurgitation occurs during isovolumic contraction. In addition, mitral regurgitation flow extends later in systole compared with aortic stenosis (during isovolumic relaxation).
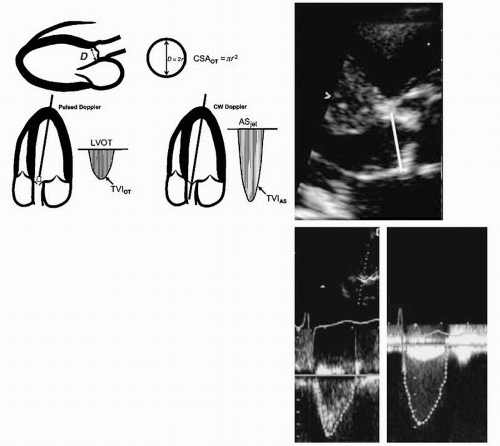
In most cases, a complete echocardiographic assessment of aortic stenosis includes a determination of aortic valve area using the continuity equation. Based on the principle of conservation of mass, the continuity equation states that the stroke volume proximal to the aortic valve (within the left ventricular outflow tract) must equal the stroke volume through the stenotic orifice. Because stroke volume is the product of the crosssectional area (CSA) and time velocity integral (TVI), the continuity equation can be arranged to yield:
This is illustrated in Figure 11.19. To calculate aortic valve area, the following three measurements must be performed: (1) the CSA of the left ventricular outflow tract (OT), (2) TVI of the outflow tract, and (3) TVI of the aortic stenosis jet (AS).
To measure the CSA of the outflow tract, the diameter of the outflow tract is generally measured from the parasternal long-axis view and the shape is assumed to be circular. The equation used is simply
where r is one half of the measured diameter (in centimeters). The importance of performing this measurement accurately cannot be overemphasized. Because the radius is squared to determine area, small errors in measuring this linear dimension will be compounded in the final formula. The smaller the annulus, the greater is the percentage error introduced by any given mismeasurement. Potential factors that may contribute to errors include image quality, annular calcification (which obscures the true dimension), a noncircular annulus (which invalidates the formula), and failure to measure the true diameter. In most cases, underestimation of true diameter is much more likely than overestimation. Thus, outflow tract diameter measurement represents an important source of error and must be measured very carefully.
FIGURE 11.19. The measurements needed to calculate aortic valve area using the continuity equation. See text for details. AS, aortic stenosis; CSA, cross-sectional area; D, diameter; TVI, time velocity integral.
The TVI of the outflow tract is measured from the apical window using pulsed Doppler imaging and positioning the sample volume just proximal to the stenotic valve. In this position, the flow is still laminar and has not yet begun to accelerate through the valve. Then, from the same transducer position, continuous wave Doppler imaging should be used to record the jet velocity envelope. Using planimetry, both envelopes can be traced so that the TVI of each can be derived. If the units used for the measurement of the outflow tract diameter are centimeters, the value of the aortic valve area will be centimeters squared. A simplified form of the continuity equation, in which maximal velocity of the outflow tract flow and valve jet are used in place of the respective TVIs, is possible because flow duration across the two sites is the same. Thus, the simplified continuity equation is
Somewhat technically easier to obtain, this equation yields valve areas that are as accurate as those obtained using the full equation (Equation 11.4).
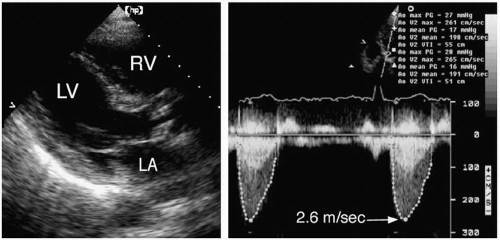
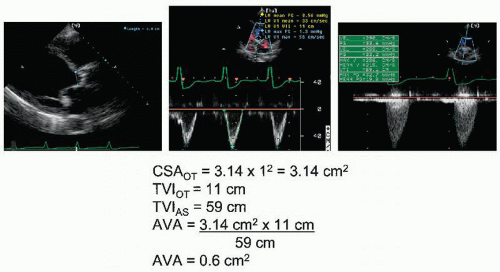
FIGURE 11.20. Aortic valve area (AVA) is calculated in a patient with aortic stenosis and severe left ventricular dysfunction. See text for details. CSA, cross-sectional area; TVI, time velocity integral.
As with the Bernoulli equation, this approach has also been validated in a variety of clinical and in vitro settings. Some of the studies validating the use of the continuity equation to measure aortic valve area are presented in Table 11.3. Thus, the continuity equation provides an accurate and reproducible assessment of the severity of aortic stenosis. It correlates well with invasive data, using the Gorlin equation. However, at very low flow rates, the correlation is not as good, with a consistent overestimation of severity of stenosis by the Gorlin equation. In addition to the challenge of properly measuring the area of the outflow tract, other potential sources of error should also be considered. It is essential that the outflow tract area and flow assessment be measured at the same level. Because the area of the outflow tract is usually measured from the parasternal long-axis view, some conventions are necessary to ensure that this is the case. In practice, the sample volume is positioned in the outflow tract from the apical window and then gradually advanced toward the aortic valve until the flow begins to accelerate. At this point, the peak velocity rises and turbulence is apparent. Then, the sample volume is gradually withdrawn toward the apex until the signal becomes laminar and without evidence of acceleration. This is the point at which the Doppler envelope should be measured.
The continuity equation has two important advantages compared with the Bernoulli equation for the assessment of aortic stenosis. First, coexisting aortic regurgitation may increase the measured transvalvular pressure gradient because of the increase in stroke volume through the valve during systole. The continuity equation, on the other hand, is not affected by the presence of aortic regurgitation. More importantly, left ventricular dysfunction may lead to reduced stroke volume and a low measured gradient even in the presence of severe valve stenosis. Again, the continuity equation is relatively unaffected and will allow an accurate determination of valve area whether the stroke volume is normal or reduced. This concept is demonstrated in Figure 11.20, which is recorded from a patient with aortic stenosis and left ventricular dysfunction. The aortic jet velocity is only 2.9 m/sec, which by the Bernoulli equation yields a peak pressure gradient of approximately 33 mm Hg. However, because the flow is reduced (as evidenced by the left ventricular outflow tract TVI of 11 cm), the calculated aortic valve area is 0.6 cm2. In this example, the severity of the aortic stenosis would have been significantly underestimated if the peak pressure gradient alone had been reported rather than the aortic valve area. Although an accurate measurement of the pressure gradient is sufficient to make clinical decisions in many cases, a determination of aortic valve area is especially important in patients with significant aortic regurgitation and/or reduced left ventricular function.
Only gold members can continue reading. Log In or Register to continue