Anatomy and Classification of Congenital Heart Disease
Paul M. Weinberg
INTRODUCTION
The hallmark of congenital heart disease is the variability in spatial relationships as well as interconnections among the various cardiac and vascular structures. To appreciate these types of abnormalities, it is first necessary to define certain terms that may have different meanings from those used to describe normal anatomy. When cardiac chambers are described, the terms right and left refer only to morphological characteristics which will be further elaborated upon below. They do not refer to the right-left frame of reference in the body. For example, right ventricle refers to a particular cardiac structure with specific morphological features, regardless of its location in the body. When the right-left frame of reference is intended, the terms right-sided or left-sided are used.
It is also important to recognize which structures are, by definition, part of a chamber and which are frequently associated with that chamber. For example, the normal right ventricle includes the infundibulum or outflow tract portion of the heart, whereas there are some hearts in which the infundibulum is partially or entirely related to the left ventricle (anatomically corrected malposition or double outlet left ventricle). Therefore, the presence of infundibulum does not define the right ventricle, but rather is usually associated with it.
Another concept that is central to a morphological approach to congenital heart disease is the recognition of the difference between anatomical, physiological, and surgical diagnoses. This chapter will concern itself entirely with anatomical descriptions and diagnoses. Some of the terms can also be used in a physiological sense; it is vital that one cannot make the mistake of using them interchangeably. For example, anatomically, transposition of the great arteries means that the aorta arises above the morphological right ventricle and the pulmonary artery above the left ventricle. This is true regardless of whether the right ventricle receives desaturated blood from the body or fully saturated blood from the lungs. Transposition physiology, however, refers to any anatomical situation in which the pulmonary artery receives blood of a higher saturation than the aorta. If a term is used without further clarification, it should always refer to anatomical diagnoses, whereas physiologic terms should always be stated as such, for example, “transposition physiology” or “physiological mitral stenosis.”
CLASSIFICATION OF CONGENITAL HEART DISEASE
Aims and Basic Principles
The purpose of a classification system is to permit the identification of all examples of anatomy, physiology, and surgery of congenital heart disease in a way that permits storage and retrieval from computerized databases. The aim of a classification system is really to classify entities, not names. As Shakespeare said, “What’s in a name? That which we call a rose by any other name would smell as sweet.” (Romeo and Juliet II, ii, 43). There seems to be a broad consensus on what the entities are. Rather than trying to win over everyone to the best nomenclature, classification systems should focus on the following five principles: (a) organization, (b) economy, (c) accuracy, (d) precision, and (e) quantification.
Organization is essential with any comprehensive classification system. Simple alphabetical listing of diagnoses is unhelpful because of the absence of a standardized nomenclature. Instead diagnoses should be grouped by the organization of the heart itself according to a systematic method. In this way, all possible diagnoses related to a given portion of the heart can be viewed at one time and the appropriate one selected. Because of the fact that there are different schools of thought as to organization, it is unlikely that a single standardized nomenclature will be developed in the near future. One approach to this problem is the one adopted by the International Society for Nomenclature of Paediatric and Congenital Heart Disease. This multidisciplinary group including pediatric cardiologists, cardiac surgeons, and morphologists has created the International Paediatric and Congenital Cardiac Code, which essentially maps terms from one nomenclature system to those of another so that entities will have a single numerical code or group of codes irrespective of the original terms. Inherent in this approach is acceptance of the notion that different groups may use different organizational approaches to categorize entities and may thus “arrive” at the same diagnostic entity by way of different paths. For example, our group would categorize tricuspid atresia as a form of abnormal atrioventricular alignment—specifically an abnormal atrial-to-atrioventricular valve (AVV) connection, whereas another group might think of the same entity as a form of single ventricle or univentricular heart. The path is not as important as assuring that a given entity is always coded in the same way, regardless of the approach. Because of this, definitions of entities are essential. Economy refers to saving time of the physician who determines which diagnoses to use and saving computer space with the avoidance of redundant information. This is accomplished through mutual exclusivity. Diagnoses are grouped within organizational categories into subgroups where diagnoses are mutually exclusive—only one diagnosis within that subgroup is possible. For example, only one atrial situs, one ventricular situs, one great artery situs, one atrial-to-AVV connection, one AVV-to-ventricle connection, and one ventriculo arterial alignment abnormality are possible. Additional diagnoses that are thought to relate a group of similar abnormalities are superfluous, and if ultimately shown to be incorrect (i.e., abnormalities not similar), can actually be counterproductive. Provision of redundant information during data
entry is wasteful of time as well as computer storage space.
entry is wasteful of time as well as computer storage space.
Accuracy means that a given diagnosis has the same meaning every time it is used. The meaning does not change with context. In other words, a particular anatomical ventricular septal defect (VSD) has the same designation regardless of ventriculoarterial alignment and great artery position. The atrial situs designation is the same whether there is dextrocardia or levocardia. Dependence on context complicates data retrieval, since a given diagnosis could have different meanings depending on what other diagnoses are present in each case.
Precision is the ability to classify fine anatomical detail if the information is available. Nonspecific diagnoses should only be used if more precise information is lacking. For example, a plain chest roentgenogram may indicate a right aortic arch (not further specified), but magnetic resonance imaging (MRI) or angiography may show a right aortic arch with retroesophageal diverticulum. A dilution of information would occur if only “right aortic arch” were used as the diagnosis. Whereas if one were searching for all right aortic arches, general as well as specific entities could be included.
Quantification is the option to assign an indication of severity to certain diagnoses. Sometimes the severity of a lesion is as important as the anatomical detail. While an epidemiologist may consider all VSDs of a particular type equally significant, the clinician may wish to distinguish small VSDs from large. In many cases, the designation is arbitrary but may still be useful.
Implementation—The Segmental Approach
The segmental approach to diagnosis in congenital heart disease was developed by Van Praagh to provide a systematic method for describing congenital heart defects. It fits the basic principles outlined above. Important features that distinguish Van Praagh’s segmental approach from many other systems include the following: (1) diagnoses are based on morphological analysis. While physiological correction of defects is the primary goal of cardiac surgery, it is also clear that attention to the underlying morphology is important as it influences surgical approach as well as long-term function. (2) The system is not situs-dependent; each segment is diagnosed independently. Situs-dependent systems suffer from two short-comings. If the situs is found to be different than initially thought, all of the dependent diagnoses change as well. If the situs is ambiguous or if the downstream connections are not one-to-one, as in double inlet ventricles, the concept of a situs-dependent system breaks down. (3) There is a hierarchy of diagnoses (Fig. 71.1). Those entities at the top do not change the diagnoses or nomenclature of those below, but they have greater significance: internal organization is more important than a stenotic valve in terms of classification. (4) There is a logical sequence to the analysis and description of the heart.
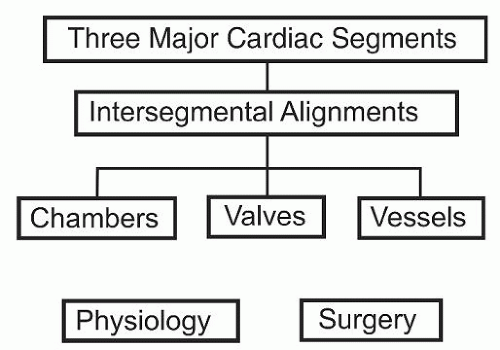 Fig. 71.1. Segmental approach hierarchy. Schematic hierarchy of cardiac diagnoses based on the segmental approach to diagnosis of Van Praagh. |
The cardiovascular system is thought of as having three major segments—viscero atrial situs, ventricular loop, and great artery situs. The situs or spatial organization of each of the segments can be described independently using morphological features of the chambers and vessels. Adjacent segments are related to each other by intersegmental alignments. The three major segments can be thought of as the blueprints of each of the floors of a three-story house. Each can be understood individually without reference to the other two, hence independence. The intersegmental alignments are analogous to stairways that connect adjacent floors.
Once segments and intersegmental alignments have been determined, individual chamber, valve, and vessel diagnoses are made. Continuing the architectural analogy, chamber, valve, and vessel abnormalities are like the furnishings of individual rooms.
Cardiac Segments
Viscero atrial situs describes the arrangement of the asymmetrical abdominal viscera and vessels, the lungs, and the atria. There are three forms of viscero atrial situs: solitus, inversus, and ambiguus. Situs solitus is characterized by a right-sided liver, left-sided stomach, and right-sided inferior vena cava (IVC). The atria display characteristic right atrial morphology of the right-sided appendage (described specifically in the “Chambers, Valves, and Vessels” section), left atrial morphology of the left-sided appendage, IVC entering the right-sided atrium, and septum primum attached to the left side of septum secundum. Situs inversus means the mirror image of solitus, viz., left-sided liver and IVC, right-sided stomach, right atrial appendage on the left, left atrial appendage on the right, IVC entering left-sided atrium, and septum primum attached to the right side of septum secundum. Situs ambiguus has characteristics of both situs solitus and situs inversus in the same person. For example, a liver that spans the abdomen from right to left (sometimes referred to as a “midline” liver) being both right-sided and left-sided has characteristics of both solitus and inversus. Similarly, bilateral morphologic right or bilateral morphologic left atrial appendages mean one solitus and one inversus. In the same way, a left-sided abdominal IVC that crosses to the right in the liver and enters a right-sided atrium with right atrial appendage morphology has features of both situs inversus (abdominal) and situs solitus (atrial). All these examples of combinations of situs solitus and situs inversus are termed situs ambiguus. This is the viscero atrial situs seen in the abdominal heterotaxy syndrome. Most, but not all, of these patients have splenic abnormalities: asplenia or polysplenia. The terms bilateral right sidedness and bilateral left sidedness are conveniences for remembering the constellation of abnormalities frequently seen with asplenia (bilateral right sidedness, since the normal right side has no spleen) or polysplenia (bilateral left sidedness, since the normal left side has a spleen, so multiple spleens is like multiple left sides), but do not carry the force of viscero atrial situs since there are numerous exceptions to the symmetry implied by those terms.
Ventricular loop is the designation for the situs of the ventricles. There are two types: D loop and L loop. Unlike the atria that are virtually always side-by-side, the ventricles, while frequently so, may be oriented antero posteriorly or supero inferiorly, still displaying one of two internal spatial organizations. Therefore, a designation independent of a simple right-left frame of
reference is necessary. Just as it is possible to distinguish a right hand from a left hand without seeing the attachment to the rest of the body, that is, without a right-left frame of reference, so too it is possible to distinguish the two stereoisomers of ventricular organization. By focusing on ventricular inflow, outflow, and septum, it is possible to attribute chirality or handedness to the ventricular organization (Fig. 71.2). If one holds his hand with the thumb, index finger, and middle finger mutually orthogonally, with the thumb representing ventricular inflow, the index finger, outflow, and the middle finger pointing to the septum, a right hand in the morphologic right ventricle indicates a D loop arrangement of ventricles. If the left hand fits the right ventricle, there is an L loop. Just as a right hand can always be distinguished from a left, so too D loop ventricles should not be mistaken for L loop ventricles regardless of the position of the heart or ventricles in three-dimensional space. What if the right ventricle does not have all three components: inflow, outflow, and septum, for example, tricuspid atresia has no right ventricular inflow? The ventricles are always concordant with each other having adjacent inflows, adjacent outflows, and a septum common to both. Because of this a right-handed right ventricle is matched with a left-handed left ventricle. Similarly, a left-handed right ventricle would go with a right-handed left ventricle. Therefore, in the case of tricuspid atresia one would simply determine the handedness of the left ventricle and interpret the ventricular loop as just described.
reference is necessary. Just as it is possible to distinguish a right hand from a left hand without seeing the attachment to the rest of the body, that is, without a right-left frame of reference, so too it is possible to distinguish the two stereoisomers of ventricular organization. By focusing on ventricular inflow, outflow, and septum, it is possible to attribute chirality or handedness to the ventricular organization (Fig. 71.2). If one holds his hand with the thumb, index finger, and middle finger mutually orthogonally, with the thumb representing ventricular inflow, the index finger, outflow, and the middle finger pointing to the septum, a right hand in the morphologic right ventricle indicates a D loop arrangement of ventricles. If the left hand fits the right ventricle, there is an L loop. Just as a right hand can always be distinguished from a left, so too D loop ventricles should not be mistaken for L loop ventricles regardless of the position of the heart or ventricles in three-dimensional space. What if the right ventricle does not have all three components: inflow, outflow, and septum, for example, tricuspid atresia has no right ventricular inflow? The ventricles are always concordant with each other having adjacent inflows, adjacent outflows, and a septum common to both. Because of this a right-handed right ventricle is matched with a left-handed left ventricle. Similarly, a left-handed right ventricle would go with a right-handed left ventricle. Therefore, in the case of tricuspid atresia one would simply determine the handedness of the left ventricle and interpret the ventricular loop as just described.
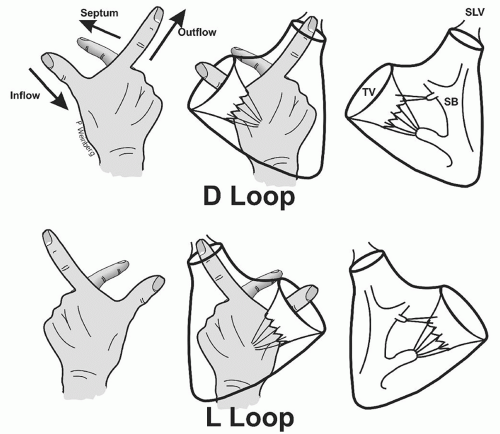 Fig. 71.2. Ventricular loop and handedness. Ventricular loop or situs is determined by the internal organization of the ventricles. Right ventricular organization shown schematically at the right is compared with the right hand; thumb, index finger, and middle finger held mutually orthogonally and representing ventricular inflow, outflow, and septum, respectively. D loop, right-hand organization of the right ventricle; L loop, left-hand organization of the right ventricle; SB, septal band; SLV, semilunar valve; TV, tricuspid valve. |
Great artery situs refers to the spatial arrangement of the semilunar valves and great arteries. A special spatial arrangement exists when the great arteries are normally aligned with the ventricles (see intersegmental connections below). Thus, a special segmental description is given in those cases where the pulmonary artery arises above the right ventricle and the aorta normally above the left ventricle. If the two great arteries spiral about each other in a clockwise manner (viewed from the ventricles) so that the ascending aorta crosses the right pulmonary artery, this is designated solitus normal great arteries. If they spiral counterclockwise with the ascending aorta crossing the left pulmonary artery, they are termed inversus normal great arteries. For all other cases—transpositions and malpositions described under intersegmental connections—the great artery segment is called D if the aortic valve is to the right of the pulmonary valve, L if the aortic valve is to the left of the pulmonary, and A if aortic valve is directly anterior (i.e., same sagittal plane) to the pulmonary.
Segmental notation: The purpose of the segmental approach to diagnosis is not only to have designations for the various spatial arrangements of the cardiac structures but also to have a concise way of communicating the basic organization of the heart when also listing the various intersegmental connections and chamber, valve, and vessel abnormalities mentioned below. This shorthand description of the cardiac organization is the segmental notation. Van Praagh conceived of each heart as representing a subset of all the possible spatial arrangements that could occur in nature. He borrowed mathematical set notation—braces { }—to accomplish this. Each heart can be described as a three-member subset of the whole with the first member of the set representing visceroatrial situs, the second, ventricular loop, and the third, great artery situs. Furthermore, the possibilities for each member of the set are designated by their first letter in capital form with the individual members separated by commas (Fig. 71.3). Therefore, the viscero atrial segment can be described by S, I, or A for situs solitus, inversus, or ambiguus. Similarly, the second member, ventricular loop, is represented by D or L for D loop or L loop organization of the ventricles. The great artery notation is S or I for solitus normal or inversus normal if the pulmonary artery arises above the right ventricle and aorta normally above the left ventricle, or D, L, or A for aortic valve to the right, left, or directly anterior relative to the pulmonary valve. In cases where the information is insufficient to determine the particular segment, that member of the subset may be represented by the letter X.
In the cases of normal arrangement of cardiac chambers and vessels, the segmental notation is {S,D,S} for visceroatrial situs solitus, ventricular D loop, and solitus normal great arteries. These would also be the segments in classical tetralogy of Fallot, and the same segmental notation would apply to classical tricuspid atresia with normally aligned great arteries. Thus, it can be seen that the segmental description does not describe abnormalities of chambers, valves, or vessels nor does it describe
intersegmental connections (except for normally aligned great arteries). Classical complete transposition of the great arteries has segments {S,D,D}, since the atria and ventricles are normally arranged, but in the absence of normally aligned great arteries the segmental notation indicates that the aorta is to the right of the pulmonary artery at the level of the semilunar valves. The same segmental description could apply to a case of double outlet right ventricle with the aorta to the right of the pulmonary artery. Classical physiologically corrected transposition of the great arteries has segments {S,L,L} indicating normal (solitus) arrangement of the atria but a ventricular L loop plus aorta to the left of pulmonary artery. Transposition of the great arteries {S,D,L} has situs solitus of viscera and atria, ventricular D loop but the transposed aorta is to the left of the pulmonary artery, rather than to the right as in the {S,D,D} form. This difference in segments does not imply different connections but rather an altered spatial arrangement, which has implications for associated abnormalities (e.g., hypoplasia of the right ventricle, straddling
tricuspid valve) as well as for surgical approaches. Figure 71.4 shows examples of spatial arrangements of atria, ventricles, and great arteries with their corresponding segmental notation. The segmental designation is a fundamental part of the overall cardiac diagnosis and is not meant to be a parenthetical, that is, extraneous or explanatory, supplement. Thus, it is incorrect to substitute parentheses () or square brackets [] for the curly braces {} used in mathematical set notation.
intersegmental connections (except for normally aligned great arteries). Classical complete transposition of the great arteries has segments {S,D,D}, since the atria and ventricles are normally arranged, but in the absence of normally aligned great arteries the segmental notation indicates that the aorta is to the right of the pulmonary artery at the level of the semilunar valves. The same segmental description could apply to a case of double outlet right ventricle with the aorta to the right of the pulmonary artery. Classical physiologically corrected transposition of the great arteries has segments {S,L,L} indicating normal (solitus) arrangement of the atria but a ventricular L loop plus aorta to the left of pulmonary artery. Transposition of the great arteries {S,D,L} has situs solitus of viscera and atria, ventricular D loop but the transposed aorta is to the left of the pulmonary artery, rather than to the right as in the {S,D,D} form. This difference in segments does not imply different connections but rather an altered spatial arrangement, which has implications for associated abnormalities (e.g., hypoplasia of the right ventricle, straddling
tricuspid valve) as well as for surgical approaches. Figure 71.4 shows examples of spatial arrangements of atria, ventricles, and great arteries with their corresponding segmental notation. The segmental designation is a fundamental part of the overall cardiac diagnosis and is not meant to be a parenthetical, that is, extraneous or explanatory, supplement. Thus, it is incorrect to substitute parentheses () or square brackets [] for the curly braces {} used in mathematical set notation.
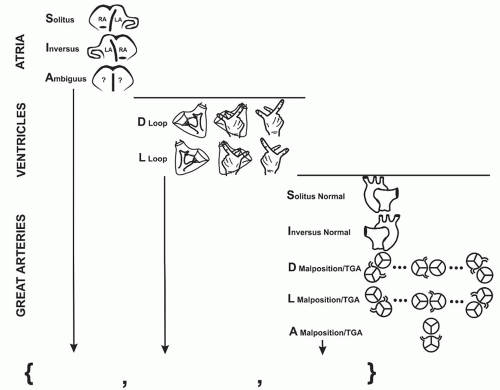 Fig. 71.3. Segmental notation. Segmental notation consists of a three-member set in braces { }. The first member is the viscero atrial situs—solitus, inversus, or ambiguus; the second is the ventricular loop—D or L; and the third is the great artery situs—solitus normal, inversus normal, D, L, or A transposition or malposition. The meaning of those terms is discussed in the text and is represented diagrammatically in the figure. Great artery situs diagrams with malposition or transposition of the great arteries in the lower right represent the two semilunar valves viewed from above; the aorta is shown with coronary arteries. LA, left atrium; RA, right atrium; ?, ambiguous morphology, a combination of solitus and inversus. |
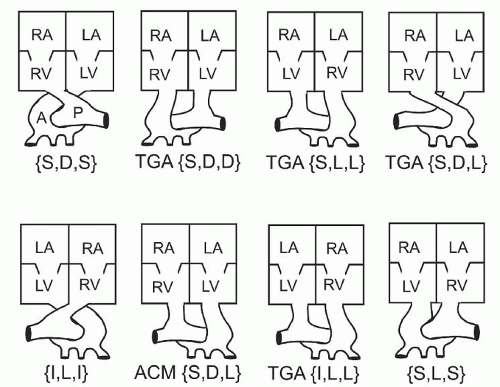 Fig. 71.4. Examples of selected anomalies and their segmental notations. Box diagrams of the heart showing the position of the atria—right atrium (RA) and left atrium (LA), the ventricles—right ventricle (RV) and left ventricle (LV), and the great arteries—aorta (A) and pulmonary artery (P). The upper left diagram represents normal spatial relations and the lower left, normal relations in situs inversus of viscera and atria. The three examples of transposition of the great arteries (TGA) in the upper row are discussed in the text. The case of anatomically corrected malposition (ACM) in the lower row has the aorta arising abnormally from a left-sided infundibulum above the left ventricle. Transposition of the great arteries {I,L,L}, physiologically complete transposition in situs inversus; {S,L,S}, isolated ventricular inversion: physiologically transposition but with normal ventriculo arterial alignment. |
INTERSEGMENTAL ALIGNMENTS
Each pair of adjacent segments has a discrete set of intersegmental alignments. Under the principle of economy described above, intersegmental alignment diagnoses are mutually exclusive entities.
Atrioventricular alignments are really a combination of atrial-to-AVV connection and AVV-to-ventricle connection. There are four basic types of atrial-to-AVV connection: two AVVs, one from each atrium; one common AVV from both atria; right AVV atresia, that is, no AVV from the right-sided atrium but one AVV from the left-sided atrium; and left AVV atresia. Each atrial-to-AVV connection has several possible AVV-to-ventricle connections:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
