The situs, or pattern of anatomic organization, of the subarterial infundibulum and of the great arteries and the degree of development of the subarterial infundibulum largely determine whether the great arteries are normally or abnormally related. There are 2 types of situs: solitus (normal) and inversus (a mirror image of solitus). Situs ambiguus means that the pattern of anatomic organization is uncertain or unknown. Infundibular development varies from absent, to atretic, to severely stenotic, to mildly or moderately stenotic; great arteries are solitus normally related or inversus normally related, respectively. When the situs of the subarterial infundibulum and the situs of the great arteries are discordant (different), then the great arteries are abnormally related. Equations indicating the situs of the infundibulum and the situs of the great arteries show whether infundibuloarterial (IA) situs concordance or discordance is present. Many types of IA anomalies typically have IA situs discordance, including transposition of the great arteries, double-outlet right ventricle, double-outlet left ventricle, and anatomically corrected malposition of the great arteries. However, tetralogy of Fallot and truncus arteriosus typically have IA situs concordance, with hypoplasia or atresia of the subpulmonary infundibulum. The relation between the great arteries in tetralogy of Fallot and in truncus arteriosus is almost normal. The IA equations demonstrate the infundibular situs, the great arterial situs, the IA situs concordance or discordance, and the degree of development of the infundibulum. The infundibular situs and the great arterial situs are the formulas or “recipes” for each of the abnormal types of conotruncal malformation.
What determines whether the great arteries are normally or abnormally related? Investigators have been trying to answer this fascinating and important question since at least 1844.
Methods
Situs is defined in Latin as layout, site, position, or situation. The plural of situs is sitūs (or situs , without a macron over the u). Situs is a fourth declension, masculine noun.
In anatomy, situs means the pattern of anatomic organization:
- (1)
situs solitus: the usual or normal anatomic pattern (noninverted) and
- (2)
situs inversus: a mirror image of situs solitus.
Situs ambiguus means an ambiguous or unknown anatomic pattern. Situs ambiguus is not a specific type of situs. Instead, it means that the type of situs (solitus or inversus) is not diagnosed. Ambiguus is correct Latin spelling; ambiguous is correct English spelling.
Infundibular situs
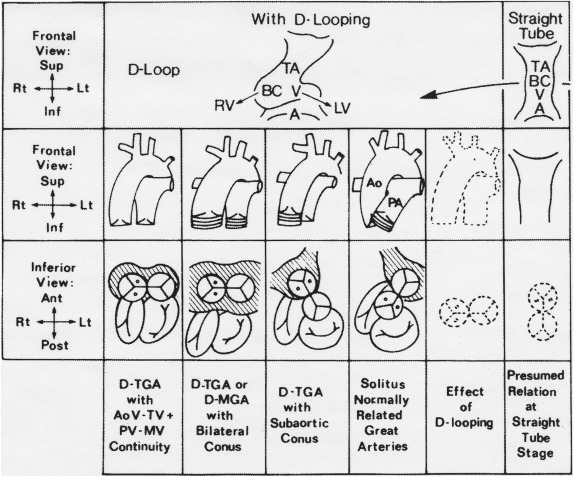
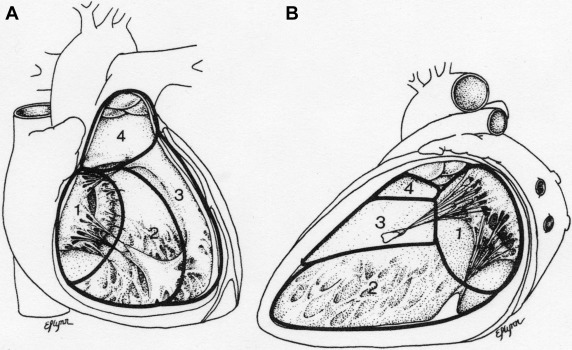
A solitus infundibulum has absence of the right-sided normally subaortic infundibular free wall musculature and well-developed left-sided normally subpulmonary infundibular free wall musculature ( Figure 1 ).
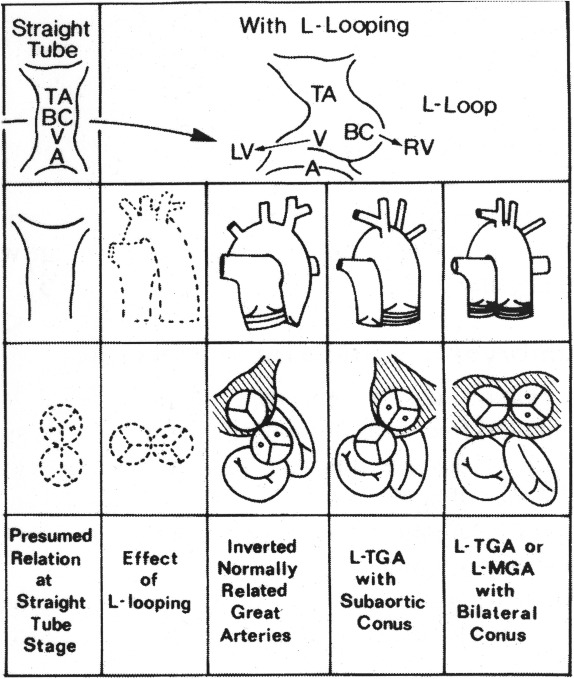
An inversus infundibulum has absence of the left-sided infundibular free wall musculature and well-developed right-sided infundibular free wall musculature ( Figure 2 ).
The infundibulum can have an ambiguous situs pattern—neither solitus nor inversus. Infundibular free wall musculature can be bilaterally present (both subaortic and subpulmonary) or bilaterally absent or very deficient (neither subaortic nor subpulmonary) ( Figure 1 ).
Situs of the great arteries
When the aortic valve (AoV) and the ascending aorta (Ao) are to the right of the pulmonary valve and the main pulmonary artery (MPA), the great arteries are in situs solitus, the noninverted pattern ( Figures 1, 3–5 ).
When the AoV and the ascending Ao are to the left of the pulmonary valve and the MPA, the great arteries are in situs inversus ( Figures 2 and 3 ).
When the AoV is directly anterior (ventral) to the pulmonary valve—neither to the right nor to the left, the great arteries are in situs ambiguus—neither solitus nor inversus.
Grading infundibular development
It is helpful to grade infundibular muscular free wall development from absent (grade 0) to well developed (grade 4).
Grade 0
Subarterial infundibular muscular free wall is absent, permitting semilunar-atrioventricular (AV) valvar direct fibrous continuity.
Grade 1
A very small amount of poorly expanded infundibular free wall is present, often resulting in outflow tract atresia.
Grade 2
A small amount of poorly expanded subarterial infundibular free wall musculature is present, often resulting in severe outflow tract stenosis.
Grade 3
Mild to moderate hypoplasia of the subarterial infundibular free wall musculature is present, typically resulting in mild to moderate outflow tract stenosis.
Grade 4
Normal or good growth of the subarterial infundibular free wall musculature is present, resulting in no outflow tract stenosis.
This grading system is useful to indicate the degree of pulmonary outflow tract obstruction in tetralogy of Fallot (TOF) and the degree of separation between the semilunar and the AV valves, as will be seen in the equations.
Results
Infundibular arterial situs equations
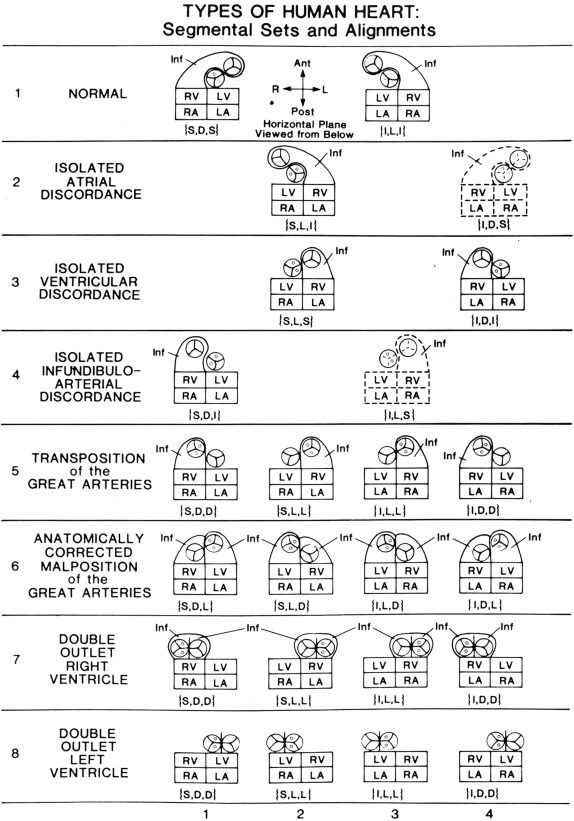
Equation 1 says: solitus normally related great arteries (SNRGA) with a segmental anatomic situs set of solitus atria, D-loop (solitus) ventricles, and SNRGA equals grade 0 (absent) development of the right-sided subaortic infundibular free wall plus grade 4 (normal) development of the left-sided subpulmonary infundibular free wall.
Which great artery is right sided and which is left sided are indicated by the great arterial symbol in the segmental anatomy: {S,D,S}. Diagrams also help: Figure 1 (third column from the right) , Figure 3 (row 1, column 1) , Figures 4 and 5 .
Equation 2 says: inverted normally related great arteries (INRGA) with a segmental anatomic situs set of inverted atria, L-loop (inverted) ventricles, and INRGA equals grade 4 (normal) right-sided development of the subpulmonary infundibular free wall myocardium plus grade 0 (absence) of the left-sided subaortic infundibular free wall myocardium. The normal inverted infundibulum is shown in Figure 2 (third column from the right) and in Figure 3 (row 1, column 3) .
Equations 1 and 2 are the frames of reference concerning the solitus normal infundibulum and the inversus normal infundibulum, respectively.
In both anatomic types of normal, the infundibular situs and the great arterial situs are both the same. Both are solitus in equation 1 , and both are inverted in equation 2 .
Thus, normally related great arteries, solitus and inversus, are characterized by infundibuloarterial (IA) situs concordance (sameness).
Transposition of the great arteries
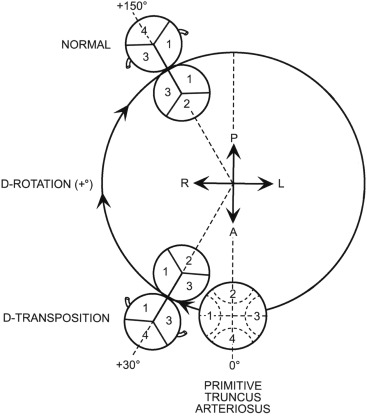
Equation 3 says: transposition of the great arteries (TGA) with the segmental anatomic situs set of solitus atria, D-loop (solitus) ventricles, and D-TGA (solitus TGA) equals a well-developed right-sided subaortic infundibular free wall plus absence of a left-sided subpulmonary infundibular free wall. D-TGA ( equation 3 ) is typical physiologically uncorrected TGA.
Typical D-TGA is depicted diagrammatically in Figure 1 (third column from the right) and in Figure 3 (row 5, column 1) .
Equation 4 says: TGA with the segmental anatomic situs set of solitus atria, L-loop (inverted) ventricles, and L-TGA (inverted TGA) equals absence of right-sided subpulmonary infundibular free wall myocardium plus a well-developed left-sided subaortic infundibular free wall. Equation 4 is typical physiologically corrected TGA.
Typical L-TGA is shown diagrammatically in Figure 2 (second column from the right) and in Figure 3 (row 5, column 2) .
Typical D-TGA ( equation 3 ) has an inverted infundibulum (4R + 0L), the same as in equation 2 , the inverted normal heart. In typical D-TGA, the great arteries are in situs solitus . Therefore, IA situs analysis in typical D-TGA is inversus-solitus, that is, discordant.
Typical L-TGA ( equation 4 ) has the reverse: a solitus infundibulum (0R + 4L), the same as in the solitus normal heart ( equation 1 ), and inverted great arteries. Therefore, IA situs analysis is solitus-inversus, that is, discordant.
Double-outlet right and left ventricles
Equation 5 represents the Taussig-Bing type of DORV, and equation 6 represents the Paul type of DOLV.
In the Taussig-Bing type of double-outlet right ventricle (DORV), both the right-sided subaortic and the left-sided subpulmonary infundibular free walls are well developed, as equation 5 indicates.
In the Paul type of double-outlet left ventricle (DOLV), there is bilateral absence of subarterial infundibular myocardium, as equation 6 indicates.
IA situs analysis in the Taussig-Bing type of DORV ( equation 5 ): ambiguus-solitus (discordant).
IA situs analysis in the Paul type of DOLV ( equation 6 ): ambiguus-solitus (discordant).
Remember that situs ambiguus is not a specific type of situs. Ambiguus means uncertain or unknown.
Anatomically corrected malposition of the great arteries
Anatomically corrected malposition of the great arteries (ACMGA) is characterized by malposition of the great arteries in which each great artery nonetheless arises above the morphologically appropriate ventricle—Ao above the morphologically left ventricle (LV), and pulmonary artery (PA) above the morphologically right ventricle (RV). This is malposition of the great arteries (Ao anterior and PA posterior), with ventriculoarterial alignment concordance. That is why this rare anomaly is called anatomically corrected malposition of the great arteries.
But how can that happen?
In all well-documented cases of ACMGA, to the best of my knowledge, the ventricles loop in 1 direction, say to the right, and the IA segment twists to the left, as in ACMGA {S,D,L} ( Figure 3 , row 6, column 1 ).
TOF and truncus arteriosus (TA) are 2 important IA anomalies that have IA situs concordance. In TOF, the great arteries are almost normally related. There is aortic-mitral fibrous continuity, but it is often tenuous (not as tight as normal), and hence, there is aortic overriding. The PA relates to the RV, but the PA is abnormally leftward, posterior, and inferior. The mild abnormality in the relation between the great arteries in typical TOF is due to hypoplasia of the subpulmonary infundibulum that results in subnormal semilunar dextrorotation. TOF is a subnormality: in the caliber of the PA outflow tract and in the degree of semilunar dextrorotation.
TOF may be represented by the following 3 equations:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


