Figure 20.2 illustrates right-bundle-branch block (RBBB) aberration of atrial premature beats (APBs). The atrial extrasystole arises after three normally conducted beats, and its impulse arrives at the right bundle branch while the latter is still refractory. The extrasystole is therefore conducted with RBBB aberration. In Figure 20.2, the seventh beat is also an extrasystole, but it is less premature and is therefore conducted normally.
RBBB aberration is much more common (about 80% of all aberration) than is left-bundle-branch block (LBBB) aberration.1,2 In an individual with cardiac disease, however, LBBB aberration constitutes a greater proportion (about 33%) of the aberrant conduction encountered. In a study by Kulbertus et al,3 in which investigators were able to produce 116 different aberrant configurations by inducing APBs in 44 patients, RBBB accounted for only 53% of the experimentally produced aberrancies—a smaller than expected proportion.
Aberrant conduction is a secondary phenomenon, always the result of some primary disturbance, and never requires treatment. At times, the morphology of the aberrant QRS complex is indistinguishable from ventricular ectopy. At other times, however, the morphologies of the QRS complexes provide hints of their having a supraventricular origin.
The first principle in the diagnosis of aberrancy is not to diagnose it unless there is evidence favoring it, because wide QRS complexes are more often produced by beats originating in the ventricular rather than in the supraventricular regions. An axiom in medical diagnosis is: “When you hear hoof beats, think first of a horse rather than a zebra—only consider a zebra if you see its stripes.” The six key characteristics of aberration (its “stripes”) are presented in Table 20.1.
The first four “stripes” are observable in Figure 20.3, in which the two continuous rhythm strips contain three clusters of rapid beats. Each cluster is initiated by a premature ectopic P wave (stripe 3). The third beat alone has a bizarre appearance (stripe 4). It has a triphasic (rsR′) RBBB pattern (stripe 1), with the initial deflection identical to that of the conducted sinus beats (stripe 2). These points clinch the recognition of aberration.
Triphasic Lead V1/V6 Morphology of the QRS Complex
The shape of the QRS complex is in many cases diagnostic of aberrancy. Triphasic contours (rsR′ in lead V1 and qRs in lead V6) heavily favor the diagnosis of aberration. Figure 20.4 illustrates an atrial tachyarrhythmia with RBBB aberration. The rsR′ pattern in lead V1 and the qRs pattern in lead V6 would each alone be virtually diagnostic of the supraventricular origin of this arrhythmia. Note that the sinus rhythm following termination of the tachyarrhythmia is rapid and irregular, as is typical with severe pulmonary disease (see Chapter 16).
Despite the availability of morphologic clues introduced during the past 40 years2,4,5 and confirmed more recently,6–9 many authors persist in ignoring them10–12 and instead continue to give predominant and undue weight to the presence or absence of independent atrial activity. When independent atrial activity (AV dissociation) is evident, it is a most valuable clue to the diagnosis of ventricular tachycardia (VT). The presence of AV dissociation cannot, however, be relied upon, for three reasons:
1. AV dissociation is present in only a minority of VTs. In one carefully studied series, it was found in only 27 of 100.13
2. Even when AV dissociation is present, the independent P waves may be difficult or impossible to recognize in the clinical tracing.
3. Rarely, junctional tachyarrhythmias with bundle-branch block may be dissociated from an independent sinus rhythm (see Fig. 20.4).
Initial Deflection of the Abnormal Beat Is Identical to Normal Beat
There is no reason for a ventricular impulse to produce an initial deflection identical to that of a normally conducted supraventricular impulse. Conversely, because normal ventricular activation begins on the left side, RBBB does not interfere with initial activation unless there is also block in one fascicle of the left bundle. As a result, if a wide QRS complex has a pattern compatible with RBBB and begins with a deflection identical to that of conducted beats, aberration is probably the diagnosis.
Atrial Activity Immediately Preceding the Abnormal Ventricular Beat
Sometimes, the diagnosis of aberration depends on the recognition of P waves preceding the abnormal QRS complex. Figure 20.5 illustrates several paroxysms of wide QRS complexes. A careful inspection reveals, however, that each group of three abnormal ventricular beats is preceded by a premature P wave, thereby confirming the diagnosis of aberrant conduction. The wide QRS complexes should be considered triphasic because there is a downward deflection between the r and K′ waves that only sometimes penetrates below the baseline to form an S wave. Note that ventricular conduction becomes aberrant when a short, normal sinus cycle follows a long cycle that follows an APB, and returns to normal only when a long cycle after an APB follows a short cycle preceding the APB. This example also illustrates the value of recording at least two simultaneous ECG leads because the P waves in some cycles are visible only in lead V6, where there is minimal evidence of the aberrantly conducted QRS complexes.
Aberrant Beats Occurring Exclusively as the Second in a Row of Beats
The reason that only the second in a row of beats tends to be aberrant is that it is the only beat that ends a relatively short cycle preceded by a relatively long cycle (see Fig. 20.1). Because the refractory period of the conduction system is proportional to the length of the preceding ventricular cycle, the sequence of a long cycle (lengthening the subsequent refractory period) followed by a short cycle provides conditions for the development of aberration.
Alternating Patterns of Bundle-Branch Block Separated by a Single Normal Beat
When a pattern that could represent either LBBB or RBBB is separated by a single normally conducted beat from a pattern that could represent the other bundle-branch block, it should be strongly presumed that there is bilateral aberration rather than ectopy from alternate ventricles. (See text and Fig. 20.14 later in this chapter.)
Identical Wide QRS Complex Pattern Previously Diagnosed as Aberrancy
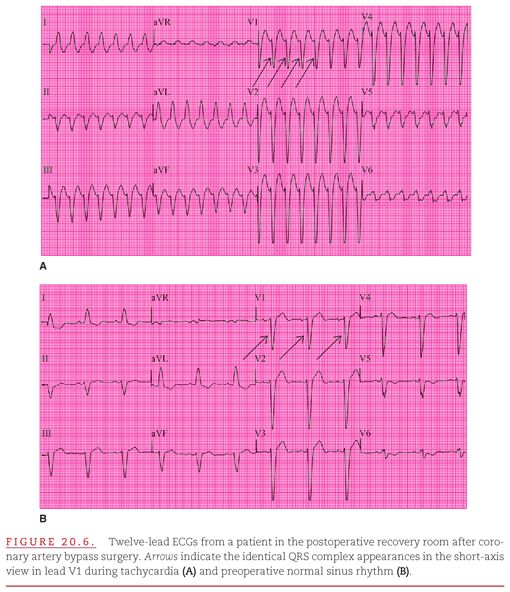
If one is lucky enough to have available a previous recording that shows the same wide QRS pattern associated with sufficient “stripes” for the diagnosis of aberrancy, the arrhythmia in question is a supraventricular tachyarrhythmia (SVT) with aberrancy. Figure 20.6A shows a tachyarrhythmia that, although the smooth downstroke in lead V1 favors left bundle branch aberrancy, could also represent right-ventricular tachycardia. Figure 20.6B is a recording from the same patient taken 1 year earlier. Because this clearly shows sinus rhythm with LBBB and the QRS complexes of the two recordings are identical, the current tachyarrhythmia can be considered an SVT with left bundle branch aberrancy, most likely atrial flutter with 2:1 AV block.
VENTRICULAR ABERRATION COMPLICATING ATRIAL FLUTTER/FIBRILLATION
Ventricular aberration often complicates atrial flutter/fibrillation (see Chapter 17
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


