Fig. 11.1
Thymus dissected in the neck and being retracted with silk ties
11.5.2 Mediastinal Stage
This can be further broken down into phases.
11.5.2.1 Anterior
A plane just posterior to the sternum is developed bluntly with an index finger. Once an adequate space has been made, a thoracoscopic sponge stick is then gently advanced into the mediastinum closely hugging the sternum, staying in the midline, and bluntly dissecting the thymus from the sternum down to the level of the diaphragm. Now the Rultract retractor is placed and with the skyhook attachment used to elevate the sternum [10]. The pressure bag is now deflated, allowing the anterior mediastinum to fall away from the sternum. Under direct or thoracoscopic vision, the entire anterior aspect of the thymus is now bluntly dissected from the posterior aspect of the sternum, both pleural surfaces, and down to the level of the diaphragm (Fig. 11.2).
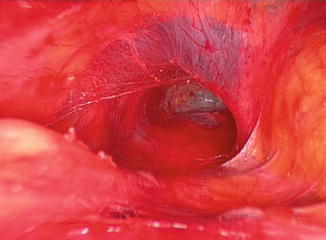
Fig. 11.2
The substernal plane
11.5.2.2 Vascular
The thymus is now retracted anteriorly and dissected sharply, posteriorly down into the mediastinum under direct vision. Blunt dissection with a peanut dissector is also effective. The gland is dissected into the mediastinum till the innominate vein is visualized. The thoracoscope is useful for illumination and occasionally for visualization at this time. The gland is dissected from the vein till the thymic veins are identified and isolated. There are usually two to three veins present opening into the anterior, inferior, or superior aspect of the vein (Fig. 11.3). The veins are doubly ligated proximally with 4–0 silk and clipped distally or ligated and divided. Clips are not used on the proximal aspect of the venous tributaries as they may dislodge during the frequent passage of instruments through the neck. Extension of the gland behind the innominate vein can be dissected free now, and the gland should be freed from the left and right innominate vein (Fig. 11.4).
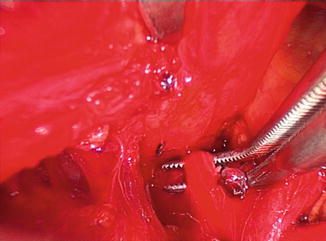
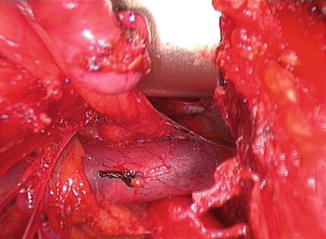
Fig. 11.3
Dissection of the thymic veins
Fig. 11.4
Dissected innominate vein
11.5.2.3 Left
The left lung is deflated and the mediastinal pleura is opened from the diaphragm to the level just below the innominate vein under thoracoscopic vision. This can be done with cautery. A thoracoscopic sucker can be used to evacuate the smoke. The operating table is rolled towards the right, which allows for increased and easier visualization of the mediastinum on the left. The left phrenic nerve is identified and the mediastinal pleura just medial to it is sharply opened inferiorly to the diaphragm and superiorly to the level of the left innominate vein (Fig. 11.5). The thymus is grasped with a thoracoscopic at a point medial to the phrenic nerve at a level below the aortopulmonary window and, using a combination of sharp and blunt dissection, resected from the pericardium. The dissection proceeds inferiorly to the diaphragm, superiorly to the innominate vein, and then as far to the right of the midline as possible. The left lung is then re-expanded.
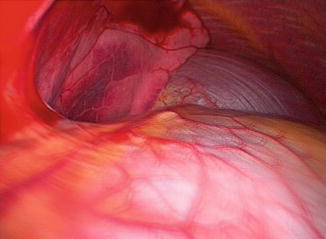
Fig. 11.5
Left pleural cavity open with visualization of the phrenic nerve
11.5.2.4 Right
The table is rolled to the left and the right lung is collapsed and the pleura opened, starting inferiorly at the diaphragm and proceeding superiorly to the innominate vein. The right phrenic nerve is visualized. The thymus is grasped medial to the nerve at the midpoint of the chest and sharply dissected to the diaphragm, to the level of the innominate vein and to the left. The gland is dissected till only the upper portion of the gland is connected to the pericardium (Fig. 11.6).
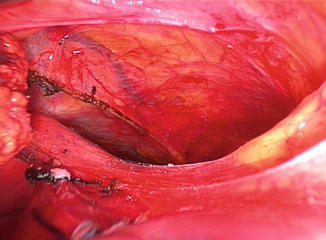
Fig. 11.6
Dissection of the right margin of the gland
11.5.2.5 Completion
The upper right lateral portion of the gland is dissected free from its pleural attachments around the superior vena cava and right innominate vein taking care to protect the phrenic nerve. This is facilitated by retracting the gland to the left using a ring clamp or an index finger. The right lung is then re-expanded. The left lung is again deflated and the gland retracted to the right. The left upper margin of the gland is dissected from the phrenic nerve and the aortopulmonary window, and the thymus is now free and removed via the cervical incision.
Any remaining anterior mediastinal fat can now be removed (Fig. 11.7). A no.19 Blake drain is placed into the mediastinum and pleural cavities through a stab incision in the neck and the left lung re-expanded. The neck incision is then closed in layers.

Fig. 11.7
Anterior mediastinum after extended thymectomy
At any time during the procedure, if exposure is not adequate to perform an extended thymectomy, then thoracoscopy via the chest should be performed to aid in the dissection and complete the intended operation.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


