Fig. 20.1
Port and robot arm placement to access shallow and deep spaces. Shallow spaces require more distance between ports at skin level
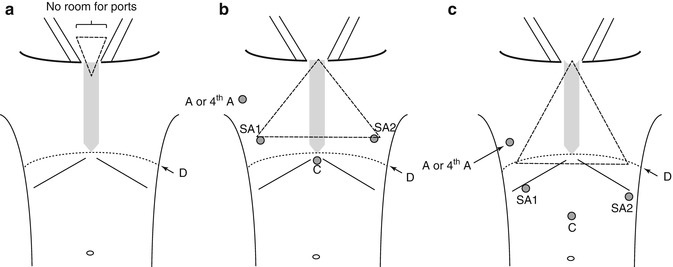
Fig. 20.2
Triangles represent currently required operative fields for the da Vinci™ robot. (a) Transcervical approach to the mediastinum: the skin surface is too small to allow docking of robotic arms. (b, c) Large operative fields to access the thorax through thoracoscopic (b) and laparoscopic (c) subxyphoid approaches (D diaphragm, C camera, SA surgeon arm, A assistant port, 4th A 4th arm [robotic])
Clinical experience with the da Vinci™ robot in the neck and thorax includes direct transcervical excision of a parapharyngeal tumor (i.e., dissection above the thoracic inlet) [1], transaxillary thyroidectomy and neck dissection [2], transthoracic mediastinal lymph node dissections [3], lobectomies [4] or thymectomies [5], and combined transthoracic robotic with transcervical approach to resect a mediastinal mass [6].
Since the da Vinci™ robot cannot be used transcervically to access the mediastinum and bilateral pleural spaces, current robotic approaches must use alternate routes. The transthoracic access is excellent for the entire mediastinum and pleural spaces, but requires single-lung ventilation and has some limitations to simultaneously approach both sides of the mediastinum. The subxyphoid approach offers outstanding visualization of both pleural spaces and the entire anterior mediastinum, but does not allow for posterior mediastinal dissection. At this time, the current version of the da Vinci™ robot is a complementary surgical option to transcervical access to the thorax. Table 20.1 summarizes a comparison of the conventional transcervical, robotic transthoracic, and robotic subxyphoid approaches to the thorax.
Table 20.1
Comparison of the conventional transcervical, robotic transthoracic, and robotic subxyphoid approaches to the thorax
Approach | Patient position | Selective ventilation | Pleural space access (complete, partial) | Mediastinal access (AS, M, P)a |
|---|---|---|---|---|
Transcervical | Supine | No | Partial | AS, M, P |
Robotic transthoracic | Supine or lateral | Yes | Complete | AS, M, P |
Robotic subxyphoid | Supine | Optional | Partial | AS |
20.3 Future Directions: Proposed Novel Robotic Approach to the Mediastinum
Our experience with thoracoscopic subxyphoid thymectomy (Figs. 20.3 and 20.4) and transdiaphragmatic thoracic surgery has led us to conceptualize the design of a robotic subxyphoid approach (Fig. 20.5a) and a robotic laparoscopic transdiaphragmatic access to the mediastinum (Fig. 20.5b). Chest insufflation with CO2 at a pressure of 8–12 mmHg helps increase the retrosternal space without the need for a sternal elevating retractor. The theoretical advantages of a subxyphoid and laparoscopic transdiaphragmatic approach over a transthoracic approach to the anterior mediastinum are bilateral visualization of phrenic nerves and avoidance of intercostal nerve pain. The retrosternal diaphragmatic defect does not require repair, while the small lateral diaphragmatic defects in the laparoscopic transdiaphragmatic approach could be easily sutured laparoscopically at the end of the procedure (Fig. 20.6). The specimen can be delivered retrosternally through a small abdominal midline incision (Fig. 20.7). The main technical disadvantage is the tangential nature of the access to the mediastinum that may limit instrument mobility.




