Fig. 14.1
Tumor of the anterior mediastinum
14.4.2 Tumors of the Superior Middle Mediastinum
The surgical technique of resection of tumors of such localization resembles the removal of the mediastinal right or left paratracheal nodes described in detail in the chapter on TEMLA. In such instances, the “older” type of technique of TEMLA is used, in which the mediastinum is dissected in the downward direction, in front of the innominate artery (on the right). It is obligatory to clearly visualize all important structures – the trachea, the esophagus, the carotid arteries, and the laryngeal recurrent nerves – before starting any dissection of the tumor (Figs. 14.2, 14.3 and 14.4). These structures should be always kept in view during dissection. Cautery or alternative devices should not be used in proximity of the laryngeal recurrent or vagus nerves.
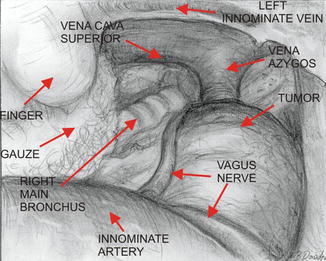
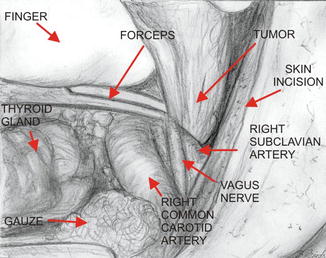
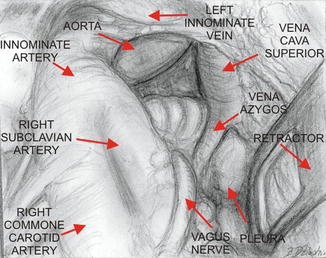
Fig. 14.2
Tumor of the right middle mediastinum (ectopic parathyroid adenoma)
Fig. 14.3
Management of the pedicle of the tumor
Fig. 14.4
View of the mediastinum after resection of the ectopic parathyroid adenoma of the right middle mediastinum
14.4.3 Tumors of the Superior Middle Mediastinum Located in the Aortopulmonary Window Area
The aortopulmonary (AP) window area is entered with the use of the technique described in the chapter on TEMLA regarding resection of nodal stations 5 and 6 (Fig. 14.5). Thanks to the recently introduced new retractors, a considerably wide access can be created which allows relatively easy dissection of tumors of this location in the semi-open fashion. All anatomical structures of the AP window area are clearly visible which makes any dissection much easier and safer.
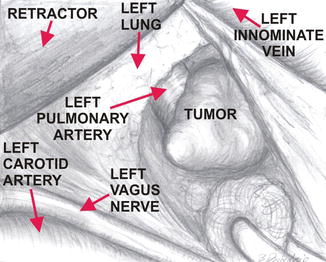
Fig. 14.5
Tumor of the aorta – pulmonary window
14.4.4 Tumors of the Superior Posterior Mediastinum
14.4.4.1 The Approach on the Left
The incision, insertion of the hook under the sternum, and elevation of the sternum are performed in the same way as was described in the chapter on TEMLA. The left carotid artery and the left laryngeal recurrent nerve are localized. An incision is made posteriorly to the left carotid artery which is retracted anteriorly. The tumor is usually accessible to palpation behind the artery, in front of the spine (Fig. 14.6). Dissection of the pedicle of the tumor is started first. The pedicle containing the nerve and the vessels should be double clipped or suture ligated. The distal part of the divided pedicle left with the tumor is used to pull the tumor up during further blind dissection with a peanut sponge. This technique usually avoids opening of the pleural cavity. The transcervical incision is usually closed without any mediastinal drainage.
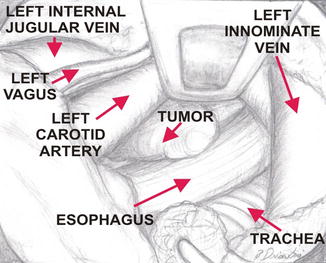
Fig. 14.6
Neurinoma of the left apex of the chest
14.4.4.2 The Approach on the Right
The incision, insertion of the hook under the sternum, elevation of the sternum, and dissection of the right vagus and laryngeal recurrent nerves are performed in the same way as was described in the chapter on TEMLA. The innominate artery is dissected and retracted superiorly and posteriorly as was described for TEMLA. Tumors of the posterior superior mediastinum are accessible to palpation in front of the spine. Resection is performed in the same way as was described for the tumors of the left posterior mediastinum (Fig. 14.7). The procedure is usually easier on the right side.
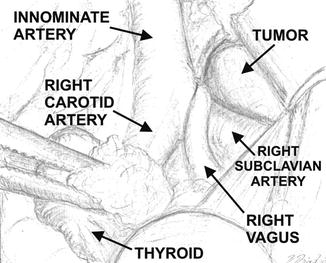
Fig. 14.7




Neurinoma of the right apex of the chest
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
