Placement of a temporary transvenous pacemaker1 can be achieved by employing any of the described central venous approaches (Figure 16.1). The decision on which approach to use depends on a variety of factors; although patient tolerability is highest with the subclavian approach, it has also the highest incidence of acute complications.2 The procedure should be performed under mild sedation, with ECG, blood pressure, and pulse oximetry monitoring.
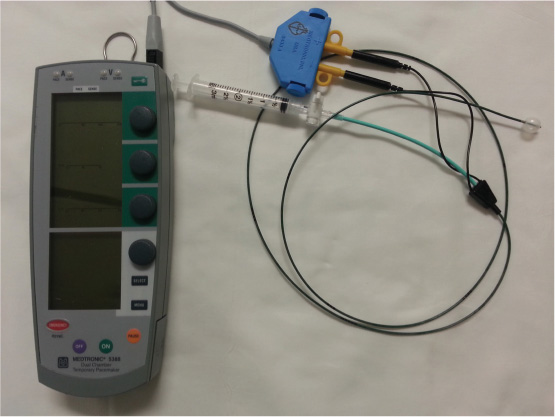
FIGURE 16.1Temporary transvenous pacemaker equipment (Medtronic, Inc., Minneapolis, MN) is shown with a temporary transvenous balloon-tipped pacing catheter (C.R. Bard, Inc., Lowell, MA).
Indications for the procedure are outlined in Table 16.1. The sole relative contraindication for the procedure is coagulopathy (INR > 1.8, PTT > 2× normal and/or platelet count < 50,000/mL).
TABLE 16.1Indications for temporary transvenous pacemaker placement.
1.Myocardial infarction complicated by:
2.Hemodynamically significant bradycardia 3.Overdrive pacing for termination of certain types of arrhythmias (type I atrial flutter, AV-nodal reentry tachycardia) 4.Bridge to permanent pacing 5.Acute complete AV block secondary to sarcoidosis or myocarditis 6.Prophylactic, in anticipation of high degree AV block secondary to certain procedures (rotablation of RCA) in the catheterization laboratory |
Femoral Vein Approach
When this approach is used, the pacing catheter is advanced through the sheath for up to 15 cm, the balloon inflated, and the catheter is advanced into the RA under fluoroscopic guidance. Access to the RV usually follows the steps described in Chapter 10. If the RV has been reached by a pacing catheter creating a loop in the RA, the lead needs to be rotated to eliminate the loop, since this loop tends to point the tip of the lead upwards towards the RVOT. This placement should only be used if the catheter tip cannot be placed into the RV apex.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


