Failure to recognize ECG features consistent with acute cor pulmonale in a man with new onset syncope and dyspnea resulted in death from undiagnosed pulmonary emboli.
A 62-year-old slender, previously healthy male jogger presented to the emergency department because of a syncopal episode and the new onset of dyspnea. Physical examination was reported as unremarkable as was a chest x-ray. An electrocardiogram (ECG) was recorded ( Figure 1 ).
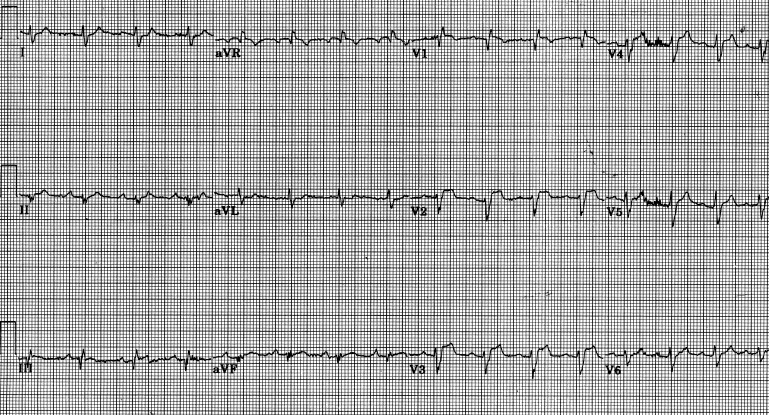
The ECG showed sinus arrhythmia at a rate of 97 beats/min, incomplete right bundle branch block with a QRS duration of 0.11 seconds, markedly delayed precordial R-wave progression with S > R in all precordial leads (so-called clockwise rotation), and ST-segment elevation in leads V 1 to V 4 . Thus, the patient had several of the electrocardiographic abnormalities that have been described in patients with pulmonary emboli ( Table 1 ).
| Rhythm | Sinus tachycardia |
| Atrial premature complexes | |
| Atrial flutter | |
| Atrial fibrillation | |
| Right ventricular premature complexes | |
| Ventricular fibrillation | |
| Pulseless electrical activity | |
| Sinus bradycardia or asystole (rarely) | |
| P waves | Rightward axis (≥75°) |
| Tall (>2.5 mm) in leads II, III, or aVF | |
| QRS complex | Right axis deviation or rightward axis shift |
| Clockwise rotation | |
| Right ventricular conduction delay (including incomplete or complete right bundle branch block) | |
| Right ventricular hypertrophy | |
| Pseudoinfarction | |
| Anterior | |
| Inferior | |
| Both | |
| ST segment | Elevation inferiorly and/or anteriorly |
| Depression | |
| T wave | Inversion anteriorly |
| Inversion inferiorly | |
| QT prolongation | |
| Pattern | S 1 Q 3 T 3 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


