Fig. 15.1
Surgical exposure of tricuspid valve
When it is scheduled one isolated tricuspid valve surgery and is certain that there is no patent foramen ovale, it is possible to perform tricuspid procedures with beating heart. Otherwise aortic crossclamping is required. For tricuspid replacement, it is preferable not to remove the leaflets in order to preserve the subvalvular apparatus.
In some cases when the leaflets are thickened and the central orifice of the valve is small, as in rheumatic degenerations, performing multiple radial incisions of the leaflets in order to increase the orifice is recommended. This will permit the largest possible prosthesis implantation. There are three techniques most commonly used to suture the prostheses along the circumference of the annulus: everting 2/0 pledgeted sutures placed from the atrial to the ventricular side of the valve, noneverting 2/0 pledgeted sutures placed from the ventricular to the atrial side of the valve, and a single continuous 2 or 3/0 polypropylene suture.
Performing the tricuspid repair procedure, the annuloplasty is performed without the involvement of the annulus in correspondence of the septal leaflet, while to perform the valve replacement, a circumferential suture is necessary. In view of this, great care is required when suturing the prostheses ring in this area in order to avoid injury to the conduction system. It is better, in the septal portion of the valve, not to touch the annulus but to use the leaflet tissue to perform the suture (Fig. 15.2).
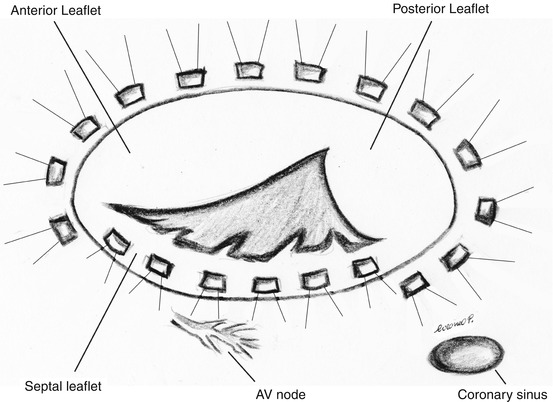
Fig. 15.2
Suture line recommended for tricuspid valve replacement
To reduce the incidence of AV block, it is possible to perform a supra-annular implantation of prosthetic valves which leaves the coronary sinus and AV node on the ventricular side of the prostheses [2] (Fig. 15.3).
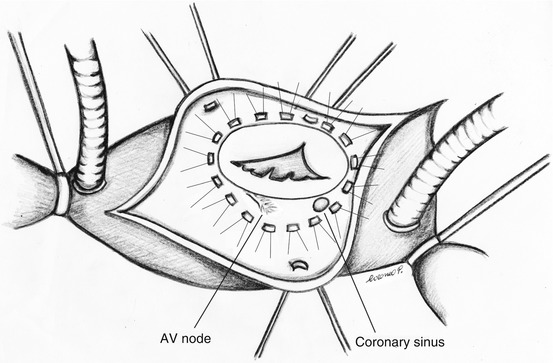
Fig. 15.3
Suture line for supra-annular prosthesis implantation
After tricuspid valve replacement, transient conduction disturbances and AV block can occur. For this, it is mandatory to place the temporary epicardial pacing wires to manage this potential event in the postoperative period. Furthermore, it is common practice to place permanent epicardial pacing wires on all patients receiving a tricuspid valve replacement putting the proximal part of the wires in a pocket on the left chest wall, in subclavicular position. This management is useful in those patients who may require permanent pacing. Particularly it would be impossible to insert transvenous pacing in presence of a mechanical prosthesis. In patients treated with bioprosthetic tricuspid valve replacement, such procedure might determine the injury of the leaflets with subsequent valve regurgitation.
For tricuspid replacement, there is no a specific prosthesis; therefore, the mitral ones are used. Whether to use, for the tricuspid valve replacement, a mechanical (Fig. 15.4) or biological prostheses valve (Fig. 15.5) remains a controversial subject.

Fig. 15.4
Mechanical prosthesis
Fig. 15.5
Biological prosthesis
The tricuspid or mitral homograft can be used as an alternative to prostheses [3, 4], although uncommon and adopted in rare cases. The use is limited by the very lack of availability, complex required surgical technique, and few results at follow-up. Nevertheless, considering its low intrinsic gradient, the fact that an anticoagulation therapy is not necessary, the potential size growth, and the resistance to infection, the homograft is an attractive option in selected pediatric patients.
Indeed, neither valve type has been shown to be a real risk factor for short- or long-term death.
15.3 Results
For tricuspid replacement, despite the progressive improvement in surgical techniques, myocardial protection, development of prosthetic materials, and medical management, there isn’t a real change in operative mortality compared with different operative eras [5].
The operative mortality ranges from 12 to 26 % [6, 7]. Emergent clinical status at surgery, advanced age, pulmonary hypertension, and NYHA class III/IV have been identified as predictive risk factors for operative mortality. Adoption of diverse valve prostheses was not associated with differences in surgery outcome [8]. Mortality increases dramatically in pediatric patients who need tricuspid valve replacement for congenital heart disease. This infrequent procedure is associated with an overall mortality of about 30 %, which increases up to 60 % in patients <1 year of age [9].
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


