Fig. 8.1
(a) AP chest radiograph in a 72-year-old male demonstrating a right-sided flail chest and multiple displaced right rib fractures. (b) 3D CT reconstruction in the same patient demonstrating multiple right-sided, posterior rib fractures with substantial displacement. (c, d, and e) Axial CT images in the same patient demonstrating multiple displaced posterior rib fractures (red arrows) and multiple minimally displaced anterolateral rib fractures (white arrows). (f) Postoperative PA chest radiograph in the same patient demonstrating fixation of multiple right-sided, posterior rib fractures performed through a posterior paramedian approach. The minimally displaced anterolateral rib fractures were not fixed
Axial and three-dimensional (3D) reconstructions of computed tomography (CT) scans of the thorax are extremely helpful in defining the location, displacement, and number of rib fractures (see Fig. 8.1) and should be obtained in all patients undergoing surgery. These images are used for preoperative planning regarding which ribs will require fixation and the location of the fractures that need to be addressed.
In the author’s experience, all rib fracture fixation can be performed using one of three surgical approaches either alone or in combination [2, 3].
1.
The lateral thoracotomy (anterior or posterior)
2.
The posterior paramedian approach
3.
The inframammary approach
It is important to recognize that ribs 1 and 2 are difficult to access surgically and fracture fixation of these ribs is generally not performed. In addition, ribs 11 and 12 are floating ribs (not structurally important) and rarely require surgical fixation.
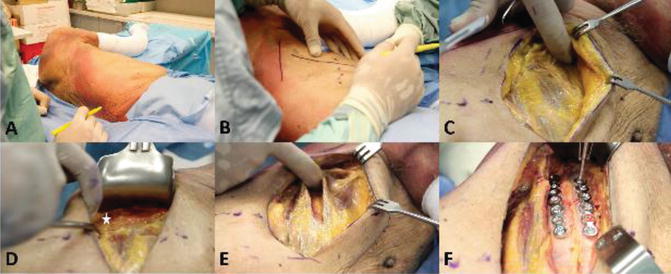
There are several steps involved in the surgical approach and rib fracture fixation that are common to all of the surgical approaches. First, the author performs the surgical preparation with the original chest tube in situ (if one has been placed) and then removes it once dissection has been carried out down to the fractured ribs and the pleural space opened. This is done to minimize the risk of developing a tension pneumothorax during induction of anesthesia and with positive pressure ventilation. The pre-existing chest tube is removed to minimize the risk of infection. Second, once dissection down to the fractured ribs is complete, the pleural space is entered through the area of greatest disruption (usually in the region of the most displaced and unstable rib fractures) using a miniature rib spreader. Irrigation and suction of the pleural space is then performed to remove any retained hemothorax (see Fig. 8.2). Deflation of the lung is not required for rib fracture fixation, and the lung can be gently retracted to allow sufficient access to the pleural space. Third, whenever possible muscle sparing approaches that utilize intermuscular intervals or split muscles in line with their fibers (rather than transecting them) are used [4, 5]. Finally, prior to closure, a new sterile, large bore (32 or 36 F) chest tube is placed through a separate incision caudal to the surgical incision and tunneled in the subcutaneous tissues to the pleural space to maximize the distance between the skin and the hardware used for rib fracture fixation.
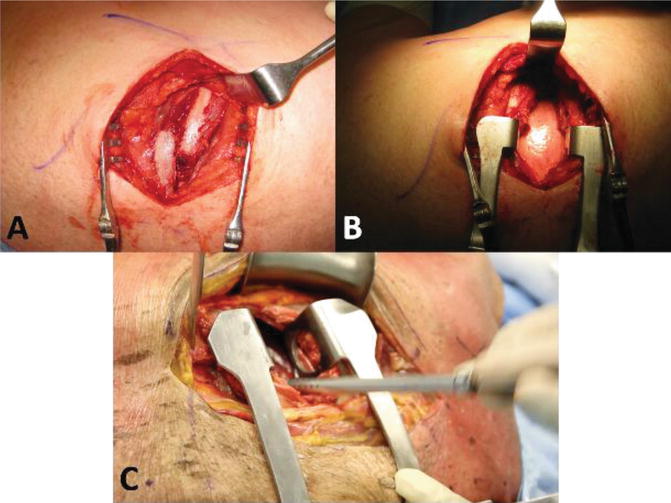
Fig. 8.2
(a and b) Intraoperative photographs of a patient undergoing rib fracture fixation surgery demonstrating displaced and overlapped rib fractures with subsequent placement of a miniature rib spreader to gain access to the pleural cavity for evacuation of hemothorax. (c) Photograph of a cadaver demonstrating suction of the pleural cavity using a pool sucker following placement of rib spreader
Lateral Thoracotomy (Anterior or Posterior) (See Figs. 8.3 and 8.4)
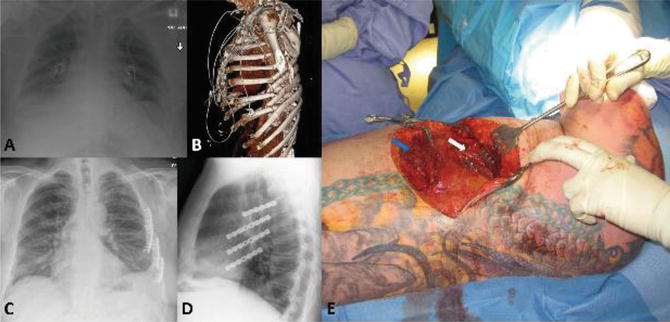
Fig. 8.3
(a) AP chest radiograph in a 48-year-old male demonstrating a left-sided flail chest and multiple displaced/comminuted anterolateral rib fractures. (b) 3D CT reconstruction in the same patient demonstrating multiple left-sided, anterolateral rib fractures with substantial displacement/comminution. (c and d) Postoperative PA and lateral chest radiograph in the same patient demonstrating fixation of multiple left-sided, anterolateral rib fractures performed through an anterolateral approach. (e) Intraoperative photograph demonstrating the anterolateral approach in this patient for fixation of anterolateral rib fractures. Muscle-splitting windows in the serratus anterior (white arrow) and external oblique (blue arrow) have been used to access rib fractures