Chapter 98 Surgical Ablation of Atrial Fibrillation
Although atrial fibrillation (AF) is often regarded as an innocuous arrhythmia, it is associated with significant morbidity and mortality secondary to its detrimental sequelae: (1) palpitations resulting in patient discomfort and anxiety; (2) loss of atrioventricular (AV) synchrony, which can compromise cardiac hemodynamics and result in various degrees of ventricular dysfunction or congestive heart failure; (3) stasis of blood flow in the left atrium, increasing the risk of thromboembolism and stroke.1–10
The following section will briefly describe the historical aspects of surgery for AF.
Historical Aspects
Left Atrial Isolation Procedure
The first procedure designed specifically to eliminate AF was first described in 1980 in the laboratory of Dr. James Cox at Duke University. The left atrial isolation procedure, which confined AF to the left atrium, restored the remainder of the heart to sinus rhythm (Figure 98-1).11 This procedure was significant because it restored a regular ventricular rate without requiring a permanent pacemaker. Since the sinoatrial (SA) node, AV node, and internodal conduction pathways are located in the right atrium and the inter-atrial septum, the left atrial isolation procedure did not affect normal AV conduction. Isolating the left atrium allowed the right atrium and the right ventricle to contract in synchrony, providing a normal right-sided cardiac output. This effectively restored normal cardiac hemodynamics.
Catheter Ablation of the Atrioventricular Node–His Bundle Complex
In 1982, Scheinman and coworkers introduced catheter fulguration of the His bundle, a procedure that controlled the irregular cardiac rhythm associated with AF and other refractory supraventricular arrhythmias.12 This procedure electrically isolated the fibrillation to the atria. Unfortunately, ablating the bundle of His required permanent ventricular pacemaker implantation to restore a normal ventricular rate.
Corridor Procedure
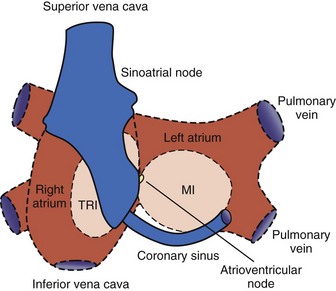
In 1985, Guiraudon et al developed the corridor procedure for the treatment of AF.13 This operation isolated a strip of atrial septum harboring both the SA node and the AV node, allowing the SA node to drive both ventricles. This procedure effectively eliminated the irregular heartbeat associated with AF, but both atria either remained in fibrillation or developed their own asynchronous intrinsic rhythm because they were isolated from the septal “corridor” (Figure 98-2). Furthermore, the atria were isolated from their respective ventricles, thereby precluding the possibility of AV synchrony. The corridor procedure was abandoned because it had no effect on the hemodynamic compromise or the risk of thromboembolism associated with AF.
Atrial Transection Procedure
In 1985, Dr. James Cox and associates described the first procedure that attempted to terminate AF.14 This was different from the earlier surgical procedures that only isolated or confined AF to a certain region of the atria. Using a canine model, Cox’s group found that a single long incision around both atria and down into the septum could terminate AF. This atrial transection procedure prevented the induction and maintenance of AF or atrial flutter in every canine that underwent the operation.15 Unfortunately, this procedure was not effective clinically and was abandoned.
Development of the Cox-Maze Procedure
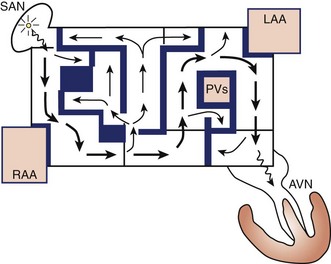
The Maze procedure was clinically introduced in 1987 by Dr. Cox after extensive animal investigation at Washington University in St. Louis.15–17 The Cox-Maze procedure was developed to interrupt any and all macro–re-entrant circuits that were felt to potentially develop in the atria, thereby precluding the ability of the atrium to flutter or fibrillate (Figure 98-3). Unlike earlier procedures, the Cox-Maze procedure successfully restored both AV synchrony and sinus rhythm, thus potentially reducing the risk of thromboembolism and stroke.18 The operation consisted of creating a myriad surgical incisions across both the right and left atria. These incisions were placed so that the SA could still direct the propagation of the sinus impulse throughout both atria. It allowed for most of the atrial myocardium to be activated, resulting in the preservation of atrial transport function in most patients.19
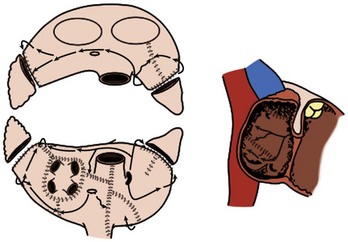
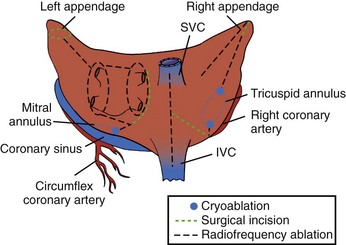
The original version, the Maze I procedure, was modified because of problems with late chronotropic incompetence and a high incidence of pacemaker implantations. The Maze II procedure, however, was extremely difficult to perform technically. It was soon replaced by the Maze III procedure, also known as the Cox-Maze III procedure today (Figure 98-4).20,21
The Cox-Maze III procedure—often referred to as the “cut-and-sew” Maze—became the gold standard for the surgical treatment of AF. In a long-term study of patients who underwent the Cox-Maze III procedure at the authors’ institution, 97% of the patients at late follow-up were free of symptomatic AF.22 These excellent results have been reproduced by other groups worldwide.23–25
The indications for surgery have been defined in a recent consensus statement.26 These presently include (1) all symptomatic patients with documented AF undergoing other cardiac surgical procedures, (2) selected asymptomatic patients with AF undergoing cardiac surgery in which the ablation can be performed with minimal risk in experienced centers, and (3) stand-alone AF, which should be considered for symptomatic patients with AF who prefer a surgical approach, have failed one or more attempts at catheter ablation, or are not candidates for catheter ablation.
In the authors’ opinion, relative indications for surgery were not included in the consensus statement. The first is a contraindication to long-term anticoagulation in patients with persistent AF and a high risk for stroke (CHADS score ≥2). Up to one third of patients with AF screened for participation in clinical trials of warfarin were deemed ineligible for chronic anticoagulation, mainly because of a perceived high risk of bleeding complications.27,28 In fact, patients on warfarin have twice the rate of intracerebral hemorrhage and mortality in a dose-dependent relationship.29 In one study, the annual rate of intracranial hemorrhage in anticoagulated patients with AF was 0.9% per year, and the overall major bleeding complications was 2.3% per year.28 The Cox-Maze procedure not only is able to eliminate AF in most patients but also amputates the left atrial appendage. The stroke rate following the procedure off anticoagulation has been remarkably low, even in patients with a CHADS score ≥2. At the authors’ institution, only 5 of 450 patients had a stroke after a mean follow-up of 6.9 ± 5.1 years. No difference in stroke rate was observed in those patients with CHADS scores above or below 2.30 This low risk of stroke following the Cox-Maze procedure has been noted in other series as well.18,31,32
Surgical treatment for AF with amputation of the left atrial appendage also should be considered in patients with chronic AF who have suffered a cerebrovascular accident despite adequate anticoagulation. These patients are at high risk of recurring neurologic events. Anticoagulation with warfarin reduces the risk of ischemic and hemorrhagic strokes by over 60% in patients with AF but does not completely eliminate this serious complication.9,33 At the authors’ institution, 20% of patients who underwent the Cox-Maze III procedure had experienced at least one episode of cerebral thromboembolism that resulted in a significant temporary or permanent neurologic deficit prior to undergoing the operation.22 No late strokes occurred in this population, with 90% of patients off anticoagulation at last follow-up.22
In patients undergoing concomitant valve surgery, studies have shown that adding the Cox-Maze procedure can decrease the late risk of cardiac-related and stroke-related deaths.34,35 However, there have been no prospective or randomized studies demonstrating the survival or other benefits of adding a Cox-Maze procedure in patients with AF. The contraindication to a Cox-Maze procedure in this group would be in asymptomatic patients who have tolerated their AF well and have not had problems with anticoagulation and in whom adding the ablation would increase their surgical risk.
Surgical Ablation Technology
For ablation technology to successfully replace incisions, it must meet several criteria. (1) It must create linear ablation lines that reliably produce bi-directional conduction block. This is the mechanism by which incisions prevent AF, by either blocking macro–re-entrant or micro–re-entrant circuits or isolating trigger foci. The authors’ laboratory and others have shown that this requires a transmural lesion, as even small gaps in ablation lines can conduct both sinus and fibrillatory impulses.36,37 (2) The ablation device must be safe. This requires a precise definition of dose-response curves to limit excessive or inadequate ablation. The surgeon must also have knowledge of the effects of a specific ablation technology on surrounding vital cardiac structures such as the coronary sinus, coronary arteries, and valvular structures. (3) The ablation device should make AF surgery simpler and require less time to perform. This would require the device to create lesions rapidly, be simple to use, and have adequate length and flexibility. (4) The device should be adaptable to a minimally invasive approach. This would include the facility to insert the device through minimal access incisions or ports, and the device should be able to create epicardial transmural lesions on the beating heart. Currently, no device has met all of these criteria. The following sections will briefly summarize the current ablation technologies and their advantages and disadvantages.
Cryoablation
Currently, two commercially available sources of cryothermal energy are being used in cardiac surgery. The older technology, based on nitrous oxide, is manufactured by AtriCure (Cincinnati, OH). More recently, ATS Medical (Minneapolis, MN.) has developed a device based on argon. At 1 atmosphere of pressure, nitrous oxide is capable of cooling tissue to −89.5° C, while argon has a minimum temperature of −185.7° C. The nitrous oxide technology has a well-defined efficacy and safety profile and is generally safe except around the coronary arteries.38,39 The potential disadvantage of cryoablation, however, is the relatively long time that is needed to create lesions (1 to 3 minutes). Creating lesions on the beating heart is also difficult because of the “heat sink” of the circulating blood volume.40 Furthermore, if blood is frozen during epicardial ablation on the beating heart, it coagulates, creating a potential risk for thromboembolism.
Radiofrequency Energy
Radiofrequency (RF) energy, which has been used for cardiac ablation for many years in the electrophysiology laboratory, was one of the first energy sources to be applied in the operating room.41 RF energy uses alternating current in the range of 100 to 1000 kHz. This frequency is high enough to prevent rapid myocardial depolarization and the induction of ventricular fibrillation, yet low enough to prevent tissue vaporization and perforation. Resistive RF energy can be delivered by either unipolar electrodes or bipolar electrodes, and the electrodes can be either dry or irrigated. With unipolar RF devices, the energy is dispersed between the electrode tip and an indifferent electrode, usually the grounding pad applied to the patient. In bipolar RF devices, alternating current is passed between two closely approximated electrodes embedded in the jaws of a clamp. The lesion size depends on electrode-tissue contact area, the interface temperature, the current and voltage (power), and the duration of delivery. The depth of the lesion can be limited by char formation, epicardial fat, myocardial and endocavity blood flow, and tissue thickness.
Numerous unipolar RF devices have been developed for ablation. These include both dry and irrigated devices and devices that incorporate suction. Although dry unipolar RF has been shown to create transmural lesions on the arrested heart in animals with sufficiently long ablation times, problems have occurred in humans. After 2-minute endocardial ablations during mitral valve surgery, only 20% of the in vivo lesions were transmural.42 Epicardial ablation on the beating heart has been even more problematic. Animal studies have consistently shown that unipolar RF is incapable of creating epicardial transmural lesions on the beating heart.43,44 Epicardial RF ablation in humans resulted in only 10% of the lesions being transmural.45 This deficiency of unipolar RF has been felt to be caused by the heat sink of the circulating blood.46 This has led some groups to examine the addition of both irrigation and suction to improve lesion formation. While these additions have improved the depth of penetration, a device capable of creating reliable transmural lesions on the beating heart is still not available.
To overcome this problem, bipolar RF clamps were developed. With bipolar RF, the electrodes are embedded in the jaws of a clamp to focus the delivery of energy. The electrodes are shielded from the circulating blood pool, and this allows for faster ablation times and limits collateral injury to tissue that is close to the electrodes. Bipolar ablation has been shown to be capable of creating transmural lesions on the beating heart, both in animals and humans, with short ablation times.47–49 Three companies (AtriCure; Medtronic, Minneapolis, MN; and Estech, San Ramon, CA) currently market bipolar RF devices.
Another advantage of bipolar RF energy is its safety profile. A number of clinical complications of unipolar RF devices that have been reported include coronary artery injuries, cerebrovascular accidents, and esophageal perforation leading to atrio-esophageal fistula.50–53 Bipolar RF technology has eliminated most of this collateral damage, and no injuries have been described with these devices despite extensive clinical use.
High-Intensity Focused Ultrasound
High-intensity focused ultrasound (HIFU) is another modality that is applied clinically for surgical ablation (St. Jude Medical, St. Paul, MN). Ultrasound effectively ablates tissue via mechanical hyperthermia. When ultrasound waves are emitted from the transducer, the resulting wave travels through the tissue causing compression, refraction, and particle movement. This translates into kinetic energy and ultimately thermal coagulative tissue necrosis. HIFU produces rapid, high-concentration energy in a focused area and is reportedly able to create transmural epicardial lesions through epicardial fat in a short time.54
Another advantage of HIFU technology is its mechanism of thermal ablation. Unlike all other energy sources that heat or cool tissue by thermal conduction, HIFU ablates tissue by directly heating the tissue in the acoustic focal volume and is therefore much less affected by the heat sink of the circulating endocardial blood pool. A few clinical studies using HIFU have shown some encouraging results.54–57 However, the efficacy of HIFU devices to reliably create transmural lesions has not been independently verified. The fixed depth of penetration of these devices may be a major problem in pathologically thickened atrial tissue. Moreover, these devices are somewhat bulky and are expensive to manufacture.
Surgical Techniques
The Cox-Maze IV Procedure
The original cut-and-sew Cox-Maze III procedure is only rarely performed today. At most centers, the surgical incisions have been replaced with lines of ablation using a variety of energy sources. At the authors’ institution, bipolar RF energy has been used successfully to replace most of the surgical incisions of the Cox-Maze III procedure. The current RF ablation–assisted procedure, termed Cox-Maze IV, incorporates the lesions as does Cox-Maze III (Figure 98-5).58 The authors’ clinical results have shown that this modified procedure has significantly shortened operative time while maintaining the high success rate of the original Cox-Maze III procedure.59
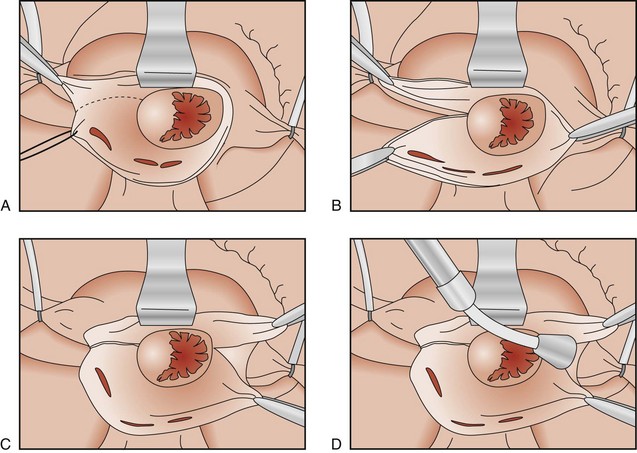
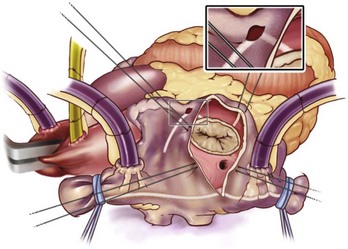
The right atrial lesion set is performed on the beating heart, as shown in Figure 98-6. A bipolar RF clamp is used to create most of the lesions. A unipolar device, either cryoablation or RF energy, is used to complete the ablation lines endocardially down to the tricuspid annulus because of the difficulty of clamping in this area.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


