Removal of IVC Filter Adherent to IVC Wall
DAVID M. WILLIAMS
Presentation
A 41-year-old woman presented in the clinic with chronic left iliac vein occlusion with left leg pain, heaviness, and swelling. She had acute left leg deep venous thrombosis (DVT) 2 months before, which was unprovoked except for the presence of May-Thurner anatomy (Fig. 1). She had a failed attempt at thrombolysis. After suspension of anticoagulation due to gastrointestinal bleeding, a Celect inferior vena cava (IVC) filter (Cook, Inc., Bloomington, IN) was placed in the infrarenal IVC. One month after her clinic visit (3 months after her DVT), she underwent successful recanalization and stenting of her left iliac common and external iliac veins. She was discharged on clopidogrel 75 mg/d, aspirin 81 mg/d, and enoxaparin 100 mg twice per day. The patient tolerated anticoagulation. Clopidogrel was discontinued after 2 months, and the patient was successfully transitioned to Coumadin. Her INR was successfully maintained between 2.2 and 3.2. Nearly 6 months after recanalization, she presented for follow-up venography to evaluate the venous stent, and requested that her filter be removed at the same time.
Assessment
In judging whether to remove a filter, we review the current indications for the filter (Table 1) as well as the anticipated difficulties in removing a filter (Table 2). According to the manufacturer’s instructions for use, the Kaplan-Meier curve of attempted retrieval of the Celect filter shows a 90% probability of successful retrieval at 1 year. At the time of venographic follow-up of her iliac vein stents, the filter would have been implanted for 8 months, and she was currently tolerating Coumadin, with an INR of 2.6. Consequently, she no longer needed the filter, and the odds of successful retrieval were considered good.
TABLE 1. When to Remove the Filter
TABLE 2. Technical Difficulty of Filter Retrieval
Initial Filter Retrieval Attempt
Filter retrieval was anticipated to be straightforward, so anticoagulation was maintained. From the right internal jugular (IJ) vein approach, a Cook retrieval loop snare was advanced into the IVC. Inferior venacavogram showed the filter retrieval hook (Fig. 1) abutting the wall of the IVC and no thrombus within the filter itself. The loop snare could not be made to engage the retrieval hook. Because the patient was anticoagulated, no aggressive attempt to secure the filter was made.
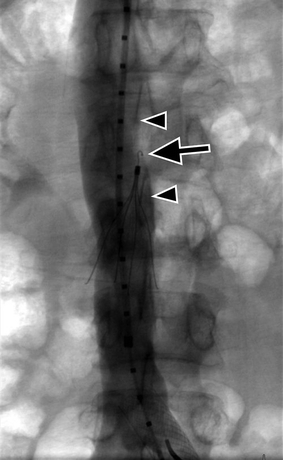
FIGURE 1 Inferior venacavogram prior to first attempt at filter retrieval, following treatment of left common iliac vein compression syndrome. The filter apex (arrow) abuts the medial wall of the IVC (arrowheads). It was not technically possible to engage the apical hook, which was embedded in the IVC wall.
Case Continued and Advanced IVC Filter Removal Techniques
The patient returned 3 months later. At this time, she had discontinued Coumadin. Her advanced D-Dimer value was 1.5 (normal 0.4 to 2.5).
From the right IJ approach, an 8 French × 45 cm sheath was placed into the IVC. Through the sheath, a recurved catheter was used to direct a wire below the hook and medial to the converging apex of the filter legs (Fig. 2), allowing the free end of the wire to be captured by a loop snare and retracted from the IJ sheath. Using firm but reasonable traction on both ends of the catheter from the jugular access, we were unable to advance the sheath over the filter hook and unable to retract the loop free of the upper body of the filter. The wire was then removed. From the right common femoral vein, an 8 × 40 balloon was directed medial to the filter and inflated, displacing the upper body of the filter laterally, in an effort to position the filter hook more centrally in the IVC lumen (Fig. 3). However, a transjugular loop snare continued to slide over the filter apex, without passing medial to the hook, suggesting that the filter hook was embedded in the IVC wall. Biopsy forceps (7 French × 55 cm Bioptome, Cordis, Bridgewater, NJ) were advanced from the 8-Fr transjugular sheath, and, after verifying proper position using rotational fluoroscopy, the opened jaws were directed onto the hook and closed (Fig. 4). Several bits of tissue were retrieved by the jaws until, after 4 passes, the hook itself was engaged. The hook was tightly grasped to allow countertraction on the filter as the sheath was advanced, closing and capturing the filter, which was then removed. Inferior venacavogram after filter retrieval showed no filling defect at the filter site, no IVC stenosis, and no contrast extravasation (Fig. 5).
Case Conclusion
The patient did well with no complication from filter extraction and required no further follow-up.



