Acute Superficial Thrombophlebitis of the Great Saphenous Vein
FEDOR LURIE
Presentation
A 58-year-old man with no history of varicose veins presents with pitting edema in his left distal calf and ankle. Measurements of his contralateral leg show a 1-cm difference in circumference at the ankle and 1.5 cm at midcalf. He reports that he had recently developed redness and pain in his left medial calf, with the redness extending to his middle thigh 2 days later. His calf is tender upon palpation, and a hard painful cord is palpable under the skin in the distal and medial thigh. He is afebrile and has no chest pain, shortness of breath, or cough.
Differential Diagnosis
The diagnosis of superficial thrombophlebitis is primarily based on the clinical presentation. The combination of pain, erythema, and tenderness in the medial thigh with a palpable tender cord in the anatomical position of the greater saphenous vein (GSV), often accompanied by a mild edema of the leg, is sufficient for establishing a clinical diagnosis.
Superficial thrombophlebitis is relatively easy to differentiate from other inflammatory conditions in the lower extremities, especially when the patient has preexisting varicose veins. It is important to exclude cellulitis that may be accompanied by lymphangitis in the medial thigh. The appearance in such cases resembles superficial phlebitis, but the patients usually have fever and general symptoms of inflammation at the onset of the disease.
When superficial phlebitis occurs in extremities without varicose veins, as in the case of this patient, an underlying condition should be suspected, with the most frequent being malignancy, thrombophilia, or vasculitis (Buerger’s, Behçet’s, and others).
Workup
A duplex ultrasound examination is performed to determine the proximal extension of the thrombus and to rule out deep vein thrombosis (DVT). The scan also confirms the diagnosis of superficial thrombophlebitis as demonstrated by an enlarged vein with endoluminal echogenic filling, absence of flow, and noncompressibility (Fig. 1).
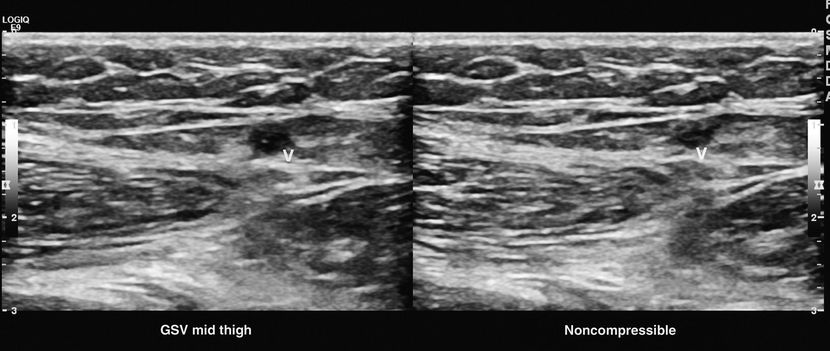
FIGURE 1 Gray scale ultrasound image of GSV. Left panel shows GSV, that in the right panel shows noncompression. This is confirmatory for a thrombosed segment.
Superficial thrombophlebitis in extremities without varicose veins is associated with malignancy in 5% to 12% and with thrombophilia in 50% of cases. Screening for malignancy may be necessary if suggestive symptoms are present. Testing for thrombophilia is not indicated unless the patient is pregnant or has a history of venous thromboembolism (VTE).
More than half of patients with Behçet’s disease are affected by superficial thrombophlebitis. The presence of erythema nodosum or inflammatory bowel disease can assist in the diagnosis of Behçet’s. When phlebitis occurs in several separate veins (thrombophlebitis saltans), or affects several segments of the same vein (thrombophlebitis migrans), a workup for Buerger’s disease is necessary.
In our patient, a duplex ultrasound scan confirmed acute thrombosis of his left GSV, with proximal extension to 10 cm from the saphenofemoral junction. He showed no evidence of DVT. Because he had a family history of venous thromboembolic disease, including a sister who had suffered multiple miscarriages, a coagulation panel was ordered, and he was positive for anti-β2-glycoprotein antibodies and factor V Leiden.
Diagnosis and Treatment
Compression therapy with bandages or graduated stockings can relieve symptoms and facilitate resolution of the thrombus. Compression therapy and ambulation alone can be sufficient treatment in as many as 80% of patients. Adding nonsteroidal anti-inflammatory drugs provides better pain relief and faster resolution of inflammation. Anticoagulation may also be beneficial. The CALISTO trial demonstrated that the risk of VTE was reduced by 85% in patients receiving 2.5 mg/d of fondaparinux compared with those receiving a placebo. However, a cost analysis has suggested that anticoagulation may not be a cost-effective option.
The American Venous Forum Guidelines recommend surgical treatment of the proximal extension of the thrombus within 1 cm from the saphenofemoral junction and conservative treatment for more distal thrombi. Surgical treatment consists of high ligation of the GSV. Stripping may be done simultaneously or delayed depending on the severity of inflammation. Revision of the saphenofemoral junction should be performed, and if thrombus extends into the common femoral vein, surgical thrombectomy may be performed.
Although there are no level 1 data comparing surgical treatment to medical management, a systematic review of six studies suggests that medical management is at least as effective as surgery. The 9th edition of the American College of Chest Physicians guidelines suggests the use of a prophylactic dose of low molecular weight heparin (LMWH) or fondaparinux for 45 days versus no anticoagulation if thrombus is at least 5 cm in length. These guideline committee also recommends medical rather that surgical treatment.
If medical management is selected for patients with proximal GSV thrombosis, a follow-up duplex scan may be necessary, especially if symptoms persist or new symptoms and signs, such as swelling or heaviness, develop. Although pulmonary embolism (PE) is a rare complication of superficial thrombophlebitis, patients should be informed of the risk and manifestations of PE.
Case Conclusion
The patient was treated with enoxaparin (Lovenox) at 1 mg/kg twice daily for 5 days and warfarin. Once his international normalized ratio (INR) was within the therapeutic range for two consecutive tests, he was managed on 5 mg of warfarin daily.



