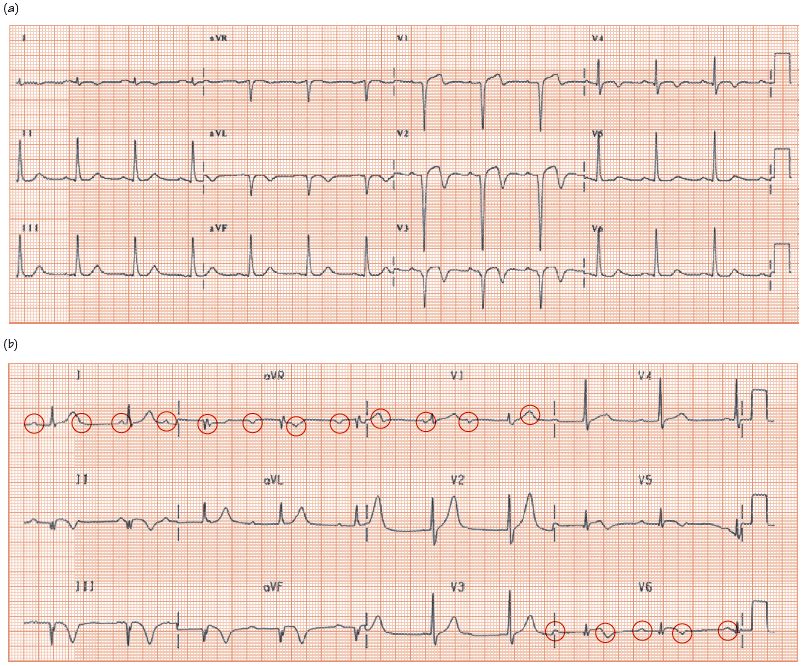
Fig. 9.2 ECGs showing Q waves. (a) Anterior wall myocardial infarct; sinus rhythm, P wave is unremarkable. Pathological Q waves in leads V1–3, really quite deep, with biphasic T waves, i.e. initially up and then down. This is a sign that the myocardial infarction (MI) causing the septal Q waves is recent, i.e. ≤ 1–7 days or so. After a few weeks the T waves become fully upright, so resuming their normal polarity. The T wave abnormality does extend more laterally, certainly into lead V4, and, albeit rather subtly, into leads V5 and V6. (b) Infero-lateral-posterior MI. This ECG is complex, with many abnormalities. Though the QRS rate is reasonable, being about 60 bpm, giving the impression that the rhythm is sinus; in fact it is not. The rhythm is complete heart block, as there is no consistent relationship between the atrial (P waves circled) and the ventricular activity. There are inferior lead (II, III, and aVF) Q waves, and the lateral leads (V5 and V6) are not nearly as tall as they should be (compare with (a) above); this is because there has also been a lateral lead infarct, resulting in the loss of much myocardium, and thus a loss of R wave height. Furthermore, lead V1 is abnormal; the main part of the QRS complex should go downwards (i.e. there should be a deep S wave). However, instead, the R wave is much larger than the S wave, a ‘so-called dominant (lead V1) R wave’, as there has also been a posterior wall MI (see Fig. 13.2). The deep inferior lead T wave inversion suggests that the MI is very recent, within the past few days (old MIs have upright ‘T’s). The extent of Q waves, loss of R wave height, and posterior MI signs suggests that the MI is very large, has affected the inferior, lateral and posterior part of the left ventricle, and is likely to be due to the occlusion of a very large right or circumflex coronary artery. Left ventricle (LV) function is likely to be poor.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


