Fig. 11.2 ECG changes in bundle branch block. (a) Normal: the septum depolarizes L → R first, both ventricles then depolarize simultaneously (endocardially to epicardially) resulting in a narrow complex QRS complex. (b) Right bundle branch block (RBBB): the septum and left ventricle depolarize normally, resulting in relatively normal QRS complexes in leads looking at the left ventricle (e.g. I, II, aVL, V4–6). The right ventricle depolarizes late, resulting in a late positive deflection in lead V1. (c) Left bundle branch block (LBBB) results in the septum being depolarized right to left (rather than the normal left to right), so there are (i) no physiological Q waves in left-sided chest leads; and (ii) delayed activation of the left ventricle, resulting in a large late positive deflection in left ventricle (LV) leads.
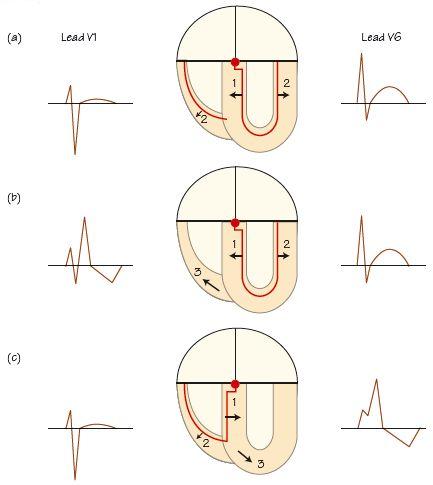
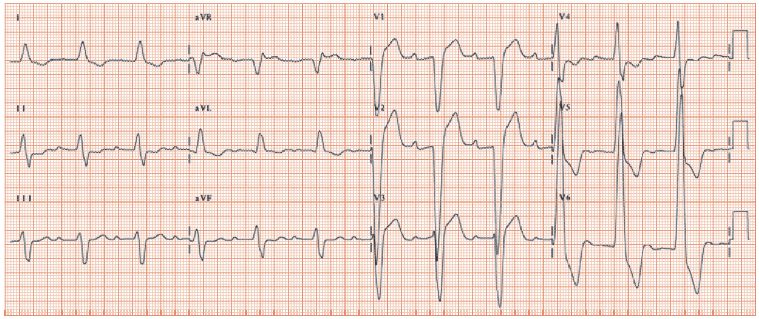
Fig. 11.3 Long PR interval. The time from the start of the P wave to the start of the QRS complex in lead V1 is 320 ms (normal PR ≤ 200 ms). This ECG also shows full left bundle branch block (LBBB), with a broad negative QRS in lead V1, very broad and positive in lead V6. Some patients with LBBB show an ‘M’ pattern in lead V6 (i.e. upwards, then a small downward deflection, then a much greater upwards deflection) – not seen here. This patient has disease affecting more than one part of the conducting system; such extensive conducting tissue disease not infrequently progresses to complete heart block.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


