Pulmonary Stenosis and Pulmonary Atresia with Intact Septum
Pulmonary Stenosis and Pulmonary Atresia with Intact Septum
Deborah J. Kozik
Mark D. Plunkett
PULMONARY STENOSIS
Pulmonary stenosis at the valvar level has been reported to account for 8% to 10% of all congenital heart defects. Although critical pulmonary stenosis may present in the newborn period and require early intervention, most of these lesions are less severe and present after the neonatal period. The pulmonary valve is usually stenotic and dome shaped with fused leaflet tissue and a small central orifice. The right ventricle is usually normal in size, but secondary hypertrophy of the ventricle and infundibulum may occur. The etiology is not known and is probably multifactorial. There is a reported increased incidence of 2% to 4% in siblings of patients with this defect. Treatment of this congenital defect with either balloon valvotomy or surgical valvotomy is associated with low morbidity and mortality and excellent long-term outcomes.
Diagnostic Considerations
Infants with critical pulmonary stenosis may present in the newborn period with severe cyanosis and heart failure. The clinical manifestations are relative to the severity of the stenosis and the patency of a foramen ovale or an atrial septal defect (ASD). In most children with pulmonary valve stenosis and intact ventricular septum, symptoms develop more slowly. Most patients are initially identified by a harsh systolic ejection murmur and a thrill over the pulmonic region on physical examination. An electrocardiogram usually reveals right-axis deviation, prominent P waves, and right ventricular (RV) hypertrophy. A chest radiograph may show prominent pulmonary artery shadows secondary to poststenotic dilation. The heart shadow is normal except in severe cases with congestive failure. Subsequent studies should include echocardiography to establish the severity of the lesion and identify associated abnormalities. Doppler evaluation allows estimation of the gradient across the valve and RV outflow tract. Finally, cardiac catheterization may be performed for additional diagnostic information, hemodynamic data, and for possible therapeutic intervention with balloon valvotomy.
Surgical Treatment and Techniques
Patients with pulmonary valve stenosis and intact ventricular septum require intervention for symptomatic lesions and for significant transvalvular pressure gradients. Historically, surgery was the mainstay of therapy for isolated pulmonary valvar stenosis. Currently, however, catheterization with balloon valvotomy has replaced surgery as the cornerstone of initial treatment. In cases of recurrent stenosis, repeat balloon valvotomy may be attempted before surgical therapy. The incidence of pulmonary insufficiency after balloon valvotomy is high (80%), but it is often clinically mild and well tolerated in most patients. Failed balloon valvotomy can be an indication for urgent surgical intervention. Surgical pulmonary valvotomy may be performed as an open technique using cardiopulmonary bypass or more rarely through a closed transventricular approach. Operative mortality is minimal except in cases of critical stenosis with associated RV hypoplasia and congestive heart failure. The results of treatment are directly related to the size of the RV chamber and the age of the patient at presentation.
Open Pulmonary Valvotomy Using Cardiopulmonary Bypass
Exposure for open pulmonary valvotomy is obtained through a median sternotomy. After heparinization, an aortic cannula is placed in the ascending aorta, and bicaval cannulation is performed. Snares are placed around the inferior and superior venae cavae. A catheter is placed in the ascending aorta for the antegrade delivery of cold blood cardioplegia. A patent ductus arteriosus must be ligated or snared at the initiation of cardiopulmonary bypass. An aortic cross-clamp is applied, and cardioplegia is delivered antegrade to achieve myocardial arrest. The snares are secured around the venous cannulae. The procedure may also be performed without a cross-clamp and cardioplegic arrest if there is no atrial or ventricular communication present.
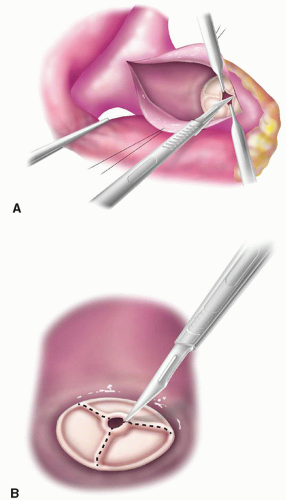
A longitudinal pulmonary arteriotomy is performed above the level of the valve commissures. The stenotic valve is inspected, and the fused commissures are identified and carefully incised with a no. 11 scalpel blade. The incisions should extend to the annulus (Fig. 91.1A, and 91.1B). Any valvar adhesions to the pulmonary arterial wall are sharply incised. A partial valvectomy may be performed to remove thickened valve tissue or dense scarring on the leaflets. Dysplastic portions of the valve may require excision. The infundibulum is then inspected through the valve for any residual subvalvular stenosis. Sharp infundibular resection through the valve should be performed if necessary. Rarely, a ventriculotomy is required with an infundibular or transannular patch closure. If a small annulus is present, a Hegar dilator may be used to size the valve annulus. The need for a transannular patch can be determined based on this measurement. If there is supravalvular hypoplasia, a pericardial patch is used to close the incision in the pulmonary artery from the annulus to the base of the left pulmonary artery. The arteriotomy is otherwise closed with a running polypropylene (prolene) suture.
If there is evidence of an ASD or patent foramen ovale, a right atriotomy is performed and the atrial septum is inspected. Closure of a patent foramen ovale or ASD is performed using primary closure or pericardial patch closure with a running prolene suture technique. The tricuspid valve (TV) leaflets are retracted to expose the infundibular outflow tract. Infundibular resection may be performed through the TV to relieve any remaining stenosis. The TV is tested for competence before closure. The atriotomy is then closed in a two-layer manner with a running prolene suture.
Fig. 91.1. (A) Open pulmonary valvotomy with division of the fused valve leaflets with a no. 11 blade scalpel or fine scissors. (B) The incision in the valve leaflet tissue should extend to the annulus.
The patient is weaned from cardiopulmonary bypass. If the right ventricle is hypoplastic, a patent foramen ovale is left partially open. Measurements of pressure in the right ventricle and the main pulmonary artery will document any residual gradient and should be performed before decannulation. Intraoperative transesophageal echocardiography is used to assess any residual gradient or pulmonary valve insufficiency. There is often a small residual gradient across the valve postoperatively, which may regress with time.
Off-Pump Transventricular Pulmonary Valvotomy
If a restrictive patent foramen ovale is present or the atrial septum is intact, pulmonary valvotomy may be performed using a closed technique that avoids the use of cardiopulmonary bypass. A wet pump should be available on standby for possible use if necessary. A median sternotomy is used, and a purse string of 4-0 prolene suture is placed on the anterior aspect of the right ventricle just below the infundibulum. A 14-gauge angiocatheter with a pressure transducer is first introduced through the right ventricle into the pulmonary artery. Hegar dilators of progressively larger sizes (up to 7 or 8 mm) are then introduced across the valve. If the membrane does not dilate easily, a long vascular clamp can be passed through the purse string and right ventricle to disrupt the valve membrane. We now prefer the use of a balloon dilation catheter with a balloon, 1 mm larger in diameter than the annulus of the pulmonary artery. The balloon can be positioned by measurement and by palpation. A needle pressure transducer is then used to assess the remaining gradient across the valve. After adequate dilation is achieved, the purse string is tied and an additional reinforcing suture is placed in the ventricular epicardium.
Perioperative Management
Most patients with pulmonary stenosis are operated on electively with routine preoperative and postoperative care. Neonates with critical stenosis should be stabilized in the intensive care unit and operated on as soon as possible. Acidosis, electrolyte abnormalities, and congestive heart failure are corrected preoperatively.
These patients may also have stenosis in the infundibular region secondary to RV myocardial hypertrophy. Inotropes must be used with caution in the preoperative and postoperative periods because increased contractility may cause increased dynamic obstruction across the pulmonary outflow tract and further compromise pulmonary blood flow.
Postoperative Care and Surgical Complications
Postoperative care for patients after surgical pulmonary valvotomy should focus on adequate RV filling pressures and reduced pulmonary artery pressures. Pulmonary vasodilators may be used in the early postoperative period to increase pulmonary flow and reduce RV afterload. Inotropic support may be useful for the first few days.
Transthoracic monitoring catheters may be placed in the right atrium or through the right ventricle into the pulmonary artery to continuously monitor hemodynamic data postoperatively. These are generally discontinued within the first 48 hours.
Pulmonary insufficiency may result from either open or closed valvotomy. Most patients will tolerate this residual valve incompetence with little difficulty. RV dysfunction may be present in the early postoperative period. This is usually transient, but may require moderate inotropic support during the early postoperative recovery.
Infants with critical pulmonary stenosis and an adequate-sized pulmonary valve annulus are often treated with balloon valvuloplasty rather than surgical intervention. However, patients with severely dysplastic pulmonary valves or significant RV outflow tract obstruction with dynamic infundibular obstruction may still come to surgical intervention and require open valvotomy or a transannular patch. If the obstruction is adequately relieved, any residual infundibular hypertrophy will regress over time. Most patients recover without complications, and long-term outcomes are excellent for both balloon valvotomy and surgical valvotomy.
PULMONARY ATRESIA WITH INTACT SEPTUM
Pulmonary atresia with intact septum (PA/IVS) is a rare defect that represents between 1% and 3% of all congenital heart defects. The exact cause or event that leads to pulmonary atresia is unknown. The lesion is sporadic, and no significant familial pattern has been identified. By definition, there is no communication between the right ventricle and the pulmonary arteries. Consequently, a patent ductus arteriosus is essential for early survival with this defect. The confluence of the branch pulmonary arteries with the main pulmonary artery is usually normal and the main pulmonary artery then tapers to an atretic pulmonary valve. The atresia of the pulmonary valve may vary significantly from a thick muscular obstruction without significant valve tissue to a thin plate-like fused trileaflet valve with well-developed sinuses and commissures. There are usually varying degrees of hypoplasia of the right ventricle and the TV, and RV-to-coronary artery fistulas may be present. Morphologically and functionally, the hypoplasia of the TV usually varies directly with the hypoplasia of the right ventricle. The TV is almost always abnormal with dysplastic leaflets, shortened chordae, and restricted leaflet motion. An Ebstein-like malformation may be present in up to 10% of patients and is usually associated with severe tricuspid regurgitation. Coronary artery fistulas are present in 45% of cases and are more common in patients with severely hypoplastic right ventricles and small competent TVs. Of note, aortopulmonary collaterals are rarely found in patients with this defect. Without early surgical intervention, children with PA/IVS have an extremely high mortality rate. The natural history of this defect is associated with 50% mortality at 2 weeks and 85% mortality at 6 months.
Diagnostic Considerations
Diagnosis of this lesion is usually made in neonates and is prompted by the presence of hypoxia in varying degrees in the newborn period. Physical examination findings are often remarkable for prominent cervical venous pulsations and hepatic enlargement. A significant murmur is indicative of tricuspid regurgitation or may be related to the patent ductus arteriosus. An electrocardiogram shows progressive evidence of right atrial enlargement with peaked right atrial P waves. A chest radiograph is unremarkable at birth but may later reveal an increased cardiac shadow secondary to right atrial and left ventricular enlargement. The diagnosis of pulmonary atresia with intact ventricular septum is usually made by two-dimensional echocardiography. Ventricular cavity sizes, valve dimensions and function, and the nature of the pulmonary artery obstruction can be determined by echocardiography. Cardiac catheterization is used for a definitive diagnosis and further evaluation. Information determined during right and left heart catheterization should include the size and competency of the TV, the functional status of the ventricles, the degree of RV hypoplasia, the degree of infundibular hypoplasia, the presence or absence of coronary sinusoids and their communications with the anatomy of the coronary arteries, and the size of the pulmonary arteries. In addition to an injection of contrast medium into the right ventricle, selective coronary angiograms are required to assess the native coronary anatomy, particularly in the severely hypoplastic RV group. Newborns with hypoxemia and poor perfusion in spite of medical management should be assessed for the presence of a restrictive ASD, which can be enlarged by balloon septostomy at the time of catheterization. If the ductus arteriosus is closed or restrictive, prostaglandin E1 (PGE1) is infused to open the ductus. In the current era, a role is developing for stenting of the ductus arteriosus at the time of catheterization as an initial palliative intervention.
Anatomic Considerations
Our initial management of patients with PA/IVS is based largely on an anatomic classification, which specifically defines the degree of RV hypoplasia and the TV annular size measured as a Z-score. This classification not only allows initial management strategies but also has predictive value for the possible use of the right ventricle in subsequent definitive biventricular repair. The Z-score is determined by comparing the diameter of the TV (as measured by echocardiography) to the “expected” size and calculating the difference in standard deviations. This allows for a quantitative assessment of the degree of hypoplasia of the TV, which in most patients varies directly with the degree of hypoplasia of the RV. We and others have found both the degree of RV hypoplasia and the TV Z-score correlate with short- and long-term outcomes of surgical management of PA/IVS.
In this classification, neonates with PA/IVS are initially separated into three groups of mild, moderate, and severe RV hypoplasia. In patients with mild RV hypoplasia, the TV and RV cavity are approximately two-thirds or greater of calculated normal size and the RV outflow tract is well developed. This usually correlates with a Z-score for the TV of 0 to -2. In patients with moderate RV hypoplasia, the TV and the RV cavity are approximately one-half of calculated normal size (with a range of one-third to two-thirds normal), and the outflow tract is developed enough to allow an effective pulmonary valvotomy. This usually correlates with a Z-score for the TV of -2 to -4. In patients with severe RV hypoplasia, the TV and RV cavity are one-third or less of calculated normal size and the outflow tract is severely hypoplastic or obliterated and is often not amenable to an effective pulmonary valvotomy. This usually correlates with a Z-score for the TV of -4 to -6. Our approach is not based on a single anatomic finding but instead assesses the overall RV morphology and the degree of both TV and RV hypoplasia.
The TV is often anatomically and functionally abnormal in patients with PA/IVS. Therefore, a TV Z-score or valve diameter alone may not adequately predict the likelihood of achieving a biventricular repair. Similarly, some patients with only moderate RV hypoplasia may have a severe tricuspid malformation and ultimately undergo a single-ventricle approach with a Glenn or Fontan procedure. In addition, the compliance of the abnormal right ventricles with significant ventricular hypertrophy and small cavity size may limit the possibility of a complete two-ventricle repair even in those with only moderate hypoplasia.
A fourth subgroup of patients may present with marked cardiomegaly caused by right atrial enlargement, severe tricuspid regurgitation, and an Ebstein’s anomaly of the TV. Dilation and dysfunction of the right atrium (RA), RV, and ventricular septal wall in these patients often compromise left ventricular function and lead to biventricular failure. These patients may have significant compromise of the left ventricle by the dilated right ventricle, and the inefficient flow of blood in and out of the right ventricle compromises overall systemic blood flow. The creation of an aortopulmonary shunt may stabilize pulmonary blood flow in these patients, but the effect of the dilated right ventricle on systemic cardiac output may remain. Patch closure of the TV is usually not suitable for these patients, because there will be no outflow of the coronary sinus return, and often sinusoidal connections and Thebesian vessels into the right ventricle cannot then be decompressed. Surgical intervention in these patients is associated with >50% mortality. In these patients, the best approach may be early cardiac transplantation.
During the initial evaluation of patients with PA/IVS, particular attention must be paid to the anatomy of the coronary circulation. Abnormalities of the coronary circulation are often found in the severely hypoplastic group and may dictate which surgical management option is indicated. During fetal development, RV hypertension may cause intramyocardial sinusoids to develop. These sinusoids often communicate by fistulas with the coronary artery circulation. The morphology of these sinusoids and their specific communications are extremely variable. Proximal coronary artery stenosis or obstruction may develop in a native coronary artery supplied by these intramyocardial sinusoids. If the distal coronary artery flow is dependent on these sinusoids for adequate myocardial perfusion, they are termed RV-dependent coronary circulations (RVDCCs). Decompression of the right ventricle in these patients is contraindicated as it may lead to acute myocardial ischemia and death. A limited experience has shown that a shunt from the aorta to the right ventricle may be beneficial in these patients to augment myocardial perfusion and coronary blood flow.
Initial Surgical Treatment and Techniques
Most infants with PA/IVS will require surgical management early in life to survive. Treatment with intravenous PGE1 will maintain pulmonary flow through the patent ductus arteriosus and allows time for evaluation and interventional decision making. Recently, some neonates have been successfully palliated with stenting of the ductus arteriosus at the time of catheterization. This has allowed delay of surgical intervention in those neonates who would otherwise be treated with a central shunt as an initial palliation. The efficacy of this catheter-based therapy appears promising for some neonates with PA/IVS, but the indications remain to be defined. Once the anatomy and morphology of these lesions have been identified at cardiac catheterization, classification is determined, and an appropriate operative strategy is planned. Delay in surgical treatment is often hazardous and may reduce survival. The primary goals of initial therapy should be to minimize early mortality and maximize the potential for a biventricular repair later in life. The choice of surgical approach is based on the anatomic classification previously described (Table 91.1).
Initial Procedures for Neonates with Mild Right Ventricular Hypoplasia
Neonates with mild RV hypoplasia (the right ventricle approximates two-thirds of normal or greater) and a tricuspid Z-score of 0 to -2 are best treated with a pulmonary valvotomy, ligation of the patent ductus arteriosus, and creation of a central systemic-to-pulmonary artery shunt. Occasionally, there are patients in which a pulmonary valvotomy alone will be adequate to restore pulmonary blood flow. These are rare and this surgical strategy should be performed with caution. Most of these patients will require a shunt as an additional source of pulmonary blood flow. Neonates with moderate RV hypoplasia and a tricuspid Z-score of -2 to -4 are treated with a pulmonary valvotomy, patch augmentation of the pulmonary outflow tract, insertion of a central shunt, and ligation of the patent ductus arteriosus. Pulmonary valvotomy with patch augmentation of the pulmonary outflow tract relieves RV hypertension, reduces tricuspid regurgitation, and promotes growth of both the RV cavity and TV. Neonates with severe RV hypoplasia and a tricuspid Z-score of -4 to -6 are usually treated with a shunt only. If there is no RVDCC and no pulmonary valvotomy is performed, then the TV can be made incompetent to decompress the RV using an open or closed tricuspid valvotomy technique. Catheter balloon disruption of the TV has also been described.
Table 91.1 Initial Surgical Management of Pulmonary Atresia with Intact Septum According to the Degree of Right Ventricular and Tricuspid Valve Hypoplasia
Classification of RV hypoplasia
RV and TV morphology
Initial treatment
Mild
Tricuspid valve Z-score 0 to -2 and RV cavity more than two-thirds of normal size, well-developed RV outflow tract
Pulmonary valvotomy with transannular patch and shunt or valvotomy only
Moderate
Tricuspid valve Z-score -2 to -4 and RV cavity one-third to two-thirds of normal size, moderately hypoplastic RV outflow tract
Pulmonary valvotomy with transannular patch and shunt
Tricuspid valve Z-score -4 to -6 and RV cavity less than one-third of normal size, severely hypoplastic or absent RV outflow tract
Shunt only; possible open or closed tricuspid valvotomy
aPatients with Ebstein malformation of the TV may be considered for heart transplant. RV, right ventricular; TV, tricuspid valve.
Off-Pump Transventricular Pulmonary Valvotomy
Closed pulmonary valvotomy may be performed on patients with mild-to-moderate RV hypoplasia who have an adequately developed RV outflow tract below the obstructed pulmonary valve. This should be performed with wet-pump standby in case there is hemodynamic instability during the procedure. The technique is performed as previously described. Many of these patients can now be effectively treated with perforation of the membrane using radiofrequency ablation catheters and subsequent balloon catheter dilation valvotomy. This approach may obviate the need for initial surgical intervention in this group of patients.
Aorta-to-Pulmonary Artery Shunt
A median sternotomy is used in performing a central shunt. The shunt insertion is performed by connecting either the innominate artery to the right pulmonary artery or the ascending aorta to the main pulmonary artery using a polytetrafluoroethylene (Gore-Tex) graft. A 3.0-mm shunt is used for neonates ≤3.0 kg, a 3.5-mm shunt in those >3.0 kg, and 4.0-mm shunt in those >4.0 kg. Cardiopulmonary bypass is usually not necessary but immediately available during the procedure. Partial occluding thin-bladed vascular C-clamps of appropriate sizes are applied to either the innominate artery or the aorta and to the pulmonary artery. Care must be taken to avoid occluding or compromising flow in the patent ductus. The arteriotomies are performed with a no. 11 scalpel blade and fine vascular scissors. The proximal anastomosis is performed on the anterior aspect of the aorta or the innominate artery in an end-to-side manner using a running 7-0 prolene suture technique. A similar anastomosis is performed to the anterior aspect of the main pulmonary artery or the right pulmonary artery. We prefer to leave the proximal clamp on during the distal anastomosis and avoid clamping the graft or allowing blood in it before flow is established. This reduces the risk of thrombus formation in the graft prior to release of the clamps. The graft is flushed with heparinized saline prior to completion of the distal anastomosis. The clamps are released slowly to deair the graft, and flow is established through the shunt. The ductus arteriosus is ligated after completion of the central shunt procedure.
Initial Procedures for Neonates with Moderate Right Ventricular Hypoplasia
Neonates with moderate RV hypoplasia are best treated with ligation of the patent ductus arteriosus, insertion of a central shunt, a pulmonary valvotomy, and patch augmentation of the pulmonary outflow tract. The transannular patch and pulmonary valvotomy may be performed with cardiopulmonary bypass and cardioplegic arrest. This allows a motionless bloodless field to perform an effective valvotomy, resect obstructing infundibular myocardium, and ensure an adequate patch augmentation. Incision of the RV outflow tract in pulmonary atresia must be performed carefully to avoid injury to the base of the aortic valve leaflet. Thus, the use of cardioplegia and cardiopulmonary bypass may allow more accurate placement of the valvotomy incision.
In select patients, we have also successfully used a closed off-pump technique to perform a pulmonary valvotomy and place a transannular outflow tract patch of pericardium without the use of either cardioplegic arrest or cardiopulmonary bypass.
Off-Pump Pulmonary Valvotomy with Transannular Right Ventricular Outflow Tract Patch
In neonates with moderate RV hypoplasia, the infundibulum may be long and narrow but reaches the pulmonary valve membrane. In these patients, a pulmonary valvotomy and a pericardial transannular patch may be performed without using cardiopulmonary bypass.
A median sternotomy incision is used. Wet-pump bypass is available with the lines on the field in case bypass is necessary. A pediatric cross-clamp is placed immediately beneath the bifurcation of the pulmonary artery. The ductus is kept patent to provide pulmonary blood flow. A vertical incision is made in the main pulmonary artery down to the atretic pulmonary valve and RV junction. A partial-thickness myocardial incision is made over the right ventricle to bring the incision over the RV cavity. Part of the muscle is resected to a depth of 1 to 2 mm to thin out the right ventricle. An elliptical pericardial patch is now sutured to the pulmonary artery incision with a running 5-0 or 6-0 prolene suture down to the RV junction. The suture line is continued onto the myocardium to the edges of the RV incision, leaving the sutures loose inferiorly. A no. 12 blade scalpel is then used to incise the pulmonary valve membrane and to cut through the remaining myocardium into the RV cavity under the pericardial patch. The sutures are pulled up to control bleeding and the cross-clamp on the pulmonary artery is removed. If the RV pressure is not adequately reduced to between one-half and one-third of systemic pressure, a rhizotomy knife is introduced through a purse string in the pericardial patch, and the RV muscle is further incised until an adequate outflow tract has been created to adequately reduce the RV pressure (Fig. 91.2A-91.2C).
Initial Procedures for Neonates with Severe Right Ventricular Hypoplasia
Neonates with severe RV hypoplasia (less than one-third normal) can be difficult to manage. If there is a restrictive atrial communication, then balloon atrial septostomy may be performed at the time of catheterization. The ductus is kept patent with PGE1 and may also be stented at the time of initial catheterization. At the time of surgery, simple pulmonary valvotomy is usually not effective in relieving RV hypertension and establishing antegrade flow to the pulmonary arteries. An extensive myomectomy and pericardial outflow tract patch may be performed using cardiopulmonary bypass. A Gore-Tex central shunt is inserted from the aorta to the main pulmonary artery, and the ductus arteriosus is ligated. If there are no sinusoids or if the sinusoids are tortuous and narrow and the native coronary circulation is normal, the right ventricle may be decompressed by incising the TV under direct vision using cardiopulmonary bypass and cardioplegic arrest or using a closed technique as described. It should be noted that patients who undergo tricuspid valvotomy decompression of the right ventricle should not have a concomitant pulmonary valvotomy with associated pulmonary insufficiency. This will allow the shunt flow to be directed retrograde across the outflow tract to the right ventricle and then into the right atrium, resulting in a significant steal of blood away from the pulmonary vascular bed. Repeat cardiac catheterization within 3 months is performed in this group of patients.
Only gold members can continue reading. Log In or Register to continue