Popliteal Entrapment in Athletes
WILLIAM D. TURNIPSEED and TRAVIS L. ENGELBERT
Presentation
Scenario #1 A 19-year-old male collegiate soccer player with progressive right leg claudication over the competitive season was seen in the clinic. Symptoms: She had limited playing time but did not affect routine activity.
Scenario #2 A 15-year-old multisport female athlete with diffuse muscle cramping affecting the proximal and distal portion of the posterior calf muscles was evaluated. Symptoms were worse when running on inclines or going up stairs, infrequently associated with plantar paresthesia.
Evaluation
Claudication is an unusual complaint in healthy athletic adolescents and young adults particularly in the absence of musculoskeletal trauma. Screening tests are indicated in order to rule out uncommon causes for exercise-induced leg pain in these individuals. Noninvasive vascular studies including resting and postexercise ankle-brachial indices (ABIs) and stress positional plethysmography are helpful for detecting vascular occlusive or impingement syndromes. These conditions include premature atherosclerosis, medial cystic arterial disease, arterial dissections, and popliteal artery entrapment. Intramuscular compartment pressures are important to consider when isolated muscle group symptoms are present since chronic exertional compartment syndromes (CECSs) can occur in active individuals and frequently coexist with functional forms of popliteal artery entrapment. EMG and nerve conduction studies are occasionally indicated to rule out peripheral nerve impingement when exercise-induced footdrop or repetitive sensory changes occur on the plantar or dorsal aspect of the feet. Vascular imaging is essential when noninvasive circulatory screening tests are positive. Our preference is use of MRI/MRA with forced plantar and dorsiflexion if popliteal artery entrapment is suspected because this technique is less invasive and musculoskeletal anatomy can be visualized and good-quality vascular images obtained in these otherwise young and healthy individuals. Vascular imaging is the only accurate means of distinguishing anatomic from functional forms of popliteal entrapment.
Testing Results
Scenario #1
Vascular screening studies performed on the male soccer player suggested occlusive disease at rest and after exercise on the right (Figure 1 and Table 1). MR angiography demonstrated a segmental occlusion of the right popliteal artery and a normal-appearing left popliteal artery (Fig. 2). Stress positional testing with forced plantar and dorsiflexion demonstrated a static short-segment occlusion of the right popliteal artery and no impingement on the left (Fig. 3). T2-weighted coronal imaging demonstrated an anomalous musculotendinous band of gastrocnemius muscle crossing the popliteal vessels bilaterally (Fig. 4).
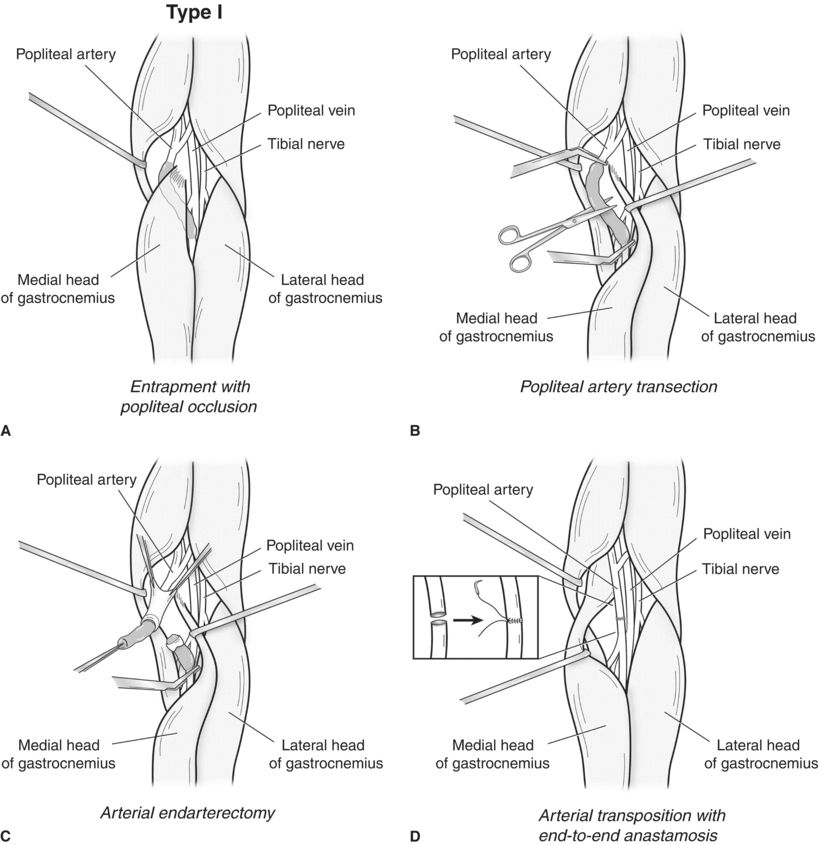
FIGURE 1 Resting ABI suggests mild occlusive change on the right. Postexercise values suggest focal occlusive change on the right consistent with ischemic claudication. The left-side values are normal. A: Type I anatomic entrapment with medial displacement and segmental occlusion of the popliteal artery is the cause for claudication in Scenario 1. B: The occluded popliteal artery is exposed through a posterior knee approach and transected. C: Eversion thromboendarterectomy is performed proximally and distally. D: The transected popliteal artery is transpositioned to its normal anatomic location and then approximated by end-to-end anastomosis.

FIGURE 2 MR angiography confirms a well- collateralized focal popliteal artery occlusion on the right and a normal left popliteal artery.

FIGURE 3 Stress positional MR angiography demonstrates static occlusion of the right popliteal artery and no evidence of impingement on the left.
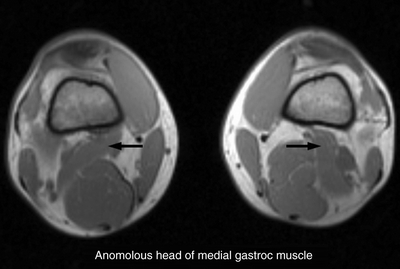
FIGURE 4 MRI imaging demonstrates anomalous gastrocnemius muscle bands bilaterally (arrows).
Scenario #2
Resting and postexercise vascular screening studies performed on the female athlete were normal (Fig. 5). However, stress positional plethysmography was markedly positive bilaterally (right > left) (Fig. 6). Neutral position MRA imaging demonstrated normal arterial positioning at rest (Fig. 7). Stress positional MRA demonstrated lateral displacement and long-segment vascular compression of the popliteal vessels bilaterally (Fig. 8A and B). Because of focal proximal muscle calf pain and cramping, compartment pressures were performed. Resting posterior superficial compartment pressures were markedly elevated at 40 mm in the posterior medial superficial and posterior lateral superficial compartments. Normal resting pressures are less than 15 mm. Although we do not routinely measure the distal deep posterior compartment pressures because of the risk of tibial neurovascular injury, distal retrotibial calf pain and plantar paresthesias can strongly suggest the presence of distal deep posterior compartment syndrome as well.
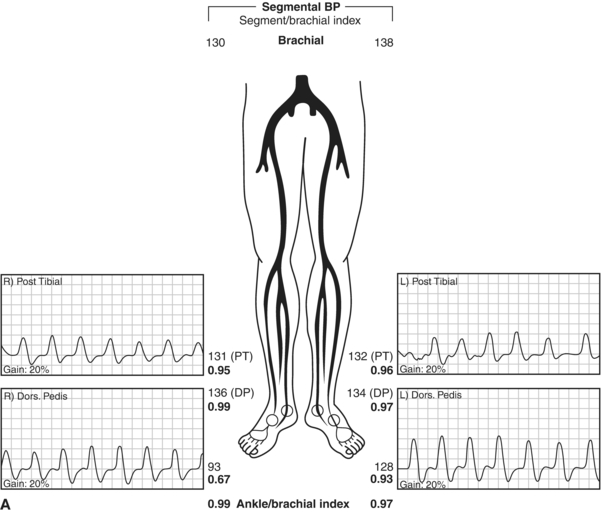
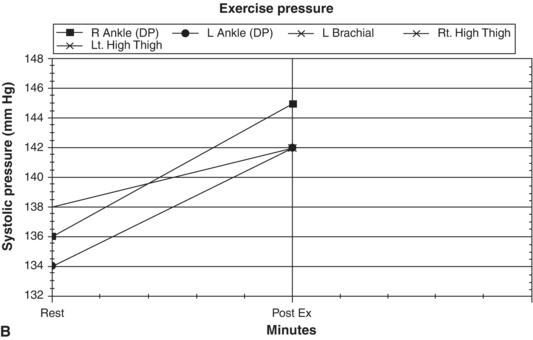
FIGURE 5 A: Resting ABIs appear normal bilaterally. B: Postexercise ABIs appear normal bilaterally.
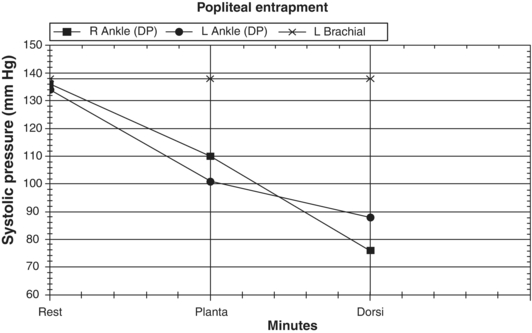
FIGURE 6 Stress positional plethysmography demonstrates popliteal artery impingement bilaterally.



