Fig. 50.2 Example of long QT interval-associated pVT. Sinus rhythm, broad low voltage P wave seen in lead II (left atrial enlargement). Mild QRS broadening, bizarre ST segments/T waves (look at the unusual T wave inversion in leads I, aVL). Very long QT interval, best seen in the first beat in the second set of leads (aVR, aVL, aVF); a pause then occurs, with further QT lengthening in the next beat. Off this beat an ectopic occurs (look at the changed shape in aVF), then a fast broad complex tachycardia, with continually changing shape – this is pVT.
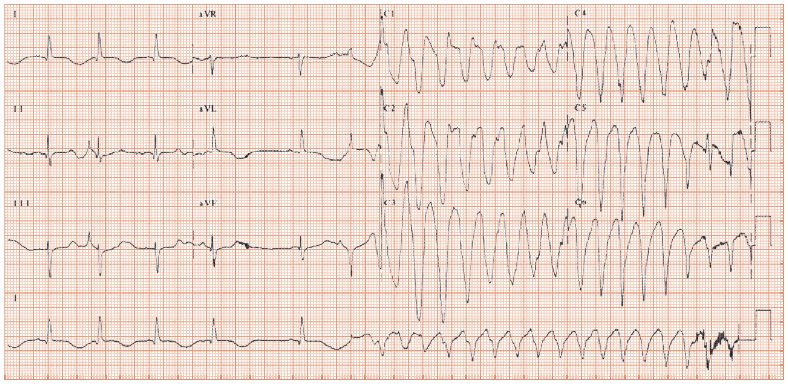
Fig. 50.3 Polymorphic ventricular tachycardia (pVT) starting during an exercise stress test. Sinus rhythm, then two ectopic beats, compensatory pause, one more sinus beat, then pVT starts, with continually changing axis (and QRS size).

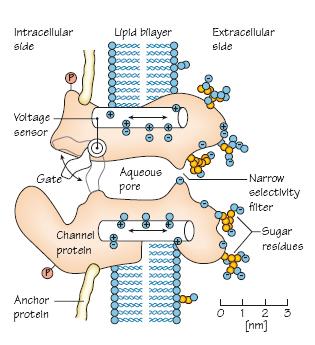
Fig. 50.4 Ion channel, emphasizing the importance of drug-channel interactions in polymorphic ventricular tachycardia.
Polymorphic (‘many shapes’) ventricular tachycardia (pVT) is common. It is underdiagnosed, as either it progresses to ventricular fibrillation (VF), cardiac arrest and sudden cardiac death (so wiping out the evidence) or it terminates spontaneously, in which case presentation is with symptoms (syncopal or near syncopal episode) but an unremarkable heart rhythm at hospitalization (e.g. sinus, atrial fibrillation). Often (not always) the clue to the diagnosis is QT interval prolongation, which underlies many cases. Other clues include finding characteristic ECGs associated with genetic channelopathies.
Pathophysiology
In monomorphic VT the pattern of spread of each beat (‘activation sequence’) is the same, whereas in pVT the activation sequence differs randomly between beats. Monomorphic VT is often ‘scar-related’, whereas pVT more often relates to (genetic or acquired) channel disorders.
ECG findings in pVT
The ECG demonstrates a broad complex tachycardia, with a continuously and randomly changing pattern (Fig. 50.1
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


