Pericardial Interventions: Pericardiocentesis, Balloon Pericardiotomy, and Epicardial Approach to Cardiac Procedures
Pericardial Interventions: Pericardiocentesis, Balloon Pericardiotomy, and Epicardial Approach to Cardiac Procedures
Mauro Moscucci
Juan F. Viles-Gonzalez
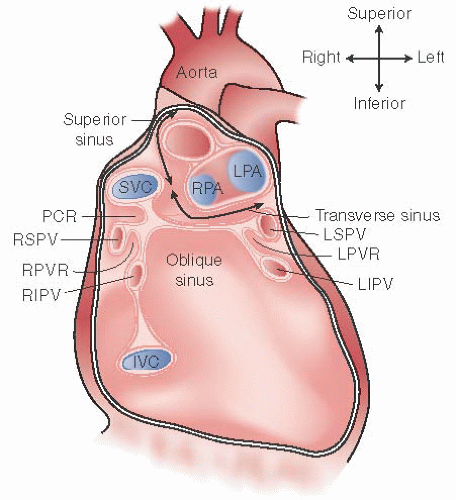
The pericardium consists of both a visceral and a parietal component, each composed of an inner layer of mesothelial cells covering an underlying fibrosa. The visceral pericardium is attached to the heart by loose connective tissue and surrounds the epicardial fat pads and coronary arteries. At the pericardial reflections, it extends onto the pulmonary veins, superior and inferior vena cavae, and several centimeters of proximal pulmonary artery and aorta, before folding around to continue as the parietal (or free) pericardium. The parietal pericardial then envelops the heart and visceral pericardium as a separate 1 to 2 mm-thick layer (Figure 38.1). The pericardial space lies between the visceral and parietal layers and normally contains 15 to 35 mL of serous pericardial fluid—an ultrafiltrate of plasma. If outward pressure is exerted by chronic pericardial effusion or cardiac chamber dilation, the pericardial layers can stretch slowly over time, but over shorter periods, the pericardium behaves as a fixed-capacity sac. Both the parietal and visceral pericardium are supplied by nerves, arteries, and lymphatics and are metabolically active, producing prostaglandin E, eicosanoids, prostacyclin, and growth factors. Inflammatory cytokines, complement myocardial cellular enzymes, and other factors may appear in the pericardial fluid in response to inflammation or transmural myocardial ischemia and necrosis, and may affect the underlying myocardium, cardiac nerves, and coronary arteries.1
The pericardial pressure is usually subatmospheric (−5 to +5 mmHg) and tracks with intrathoracic pressure during the respiratory cycle.1 During inspiration, intrapleural pressure and pericardial pressure fall more than systemic venous pressure, thus increasing the right atrial filling gradient and right ventricular stroke output (see chapter 23). In contrast, the falling intrapleural pressure during inspiration reduces pulmonary venous pressure, and decreases the left atrial filling gradient and left ventricular filling. Together with an increase in left ventricular afterload (owing to an increase in the relative difference between left ventricular end-diastolic and aortic pressure), this reduces left ventricular stroke output during inspiration. These effects are reversed during expiration. Therefore, under normal conditions, the hemodynamic effects of respiration cause cyclical changes in ventricular stroke output that are nearly 180° out of phase between the right and left ventricles.
The parietal pericardium also contributes to the diastolic compliance characteristics of the heart, especially over the thin-walled atrial and right ventricular chambers.2,3 The pericardium thus limits acute cavity dilation in situations such as right ventricular infarction, massive pulmonary embolism, and acute aortic insufficiency. If excess pericardial fluid accumulates in the pericardial space beyond its limited capacity to stretch, the pericardial pressure rises and begins to progressively compress the underlying cardiac chambers. Since this pressure is applied equally to all chambers, a rising pericardial pressure couples the diastolic behavior of the left and right ventricles together and creates ventricular interdependence whereby changes in pressure and volume in one ventricle thus produce changes in diastolic filling, contraction, and relaxation in the other ventricle.1 For example, acute increases in right ventricular size (such as in right ventricular infarction or pulmonary embolism) will increase the intrapericardial pressure, cause an increase in the stiffness of both ventricles, and reduce their compliance. Whenever right ventricular diastolic pressure exceeds left ventricular diastolic pressure, the common external pericardial constraint can cause the intraventricular septum to shift leftward and impede left ventricular filling.
Figure 38.1 The anatomy of the pericardium space and its reflections along the great vessels, sinuses, and recesses is shown in an anterior view after removal of the heart. The transverse sinus is limited by a pericardial reflection between the superior pulmonary veins. The oblique sinus is confined by the pericardial reflections around the pulmonary veins and the inferior vena cava. PCR, postcaval recess; RPA, right pulmonary artery; RPVR and LPVR, right and left pulmonary vein recesses; LPA, left pulmonary artery; SVC and IVC, superior and inferior vena cavae.
As described in detail in Chapter 44, pericardial disease can manifest with a variety of presentations, of which acute fluid accumulation leading to tamponade physiology and chronic fluid accumulation are relatively common. In addition, the growth in the performance of complex coronary interventions and catheter-based procedures for ablation of arrhythmias and for structural heart disease has been associated with an increase in coronary artery and cardiac perforation, and pericardial tamponade as a complication of these procedures.4 Thus, familiarity with elective or emergency management of pericardial effusion and tamponade continue to be important components of contemporary interventional cardiology. More recently, there has been a renewed interest in the pericardial space as a site for drug administration and as a new access site for mapping and ablation of ventricular arrhythmias. In this chapter, we will review indications and techniques of pericardiocentesis, balloon pericardiotomy, and pericardial access to the epicardium.
PERICARDIOCENTESIS
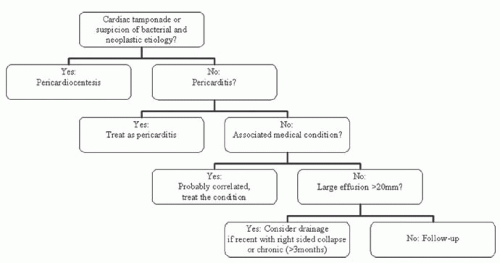
The etiology of pericardial effusion varies, and the role of pericardiocentesis in its management depends on the presence of tamponade physiology, the size of the effusion, and the ability to obtain the appropriate diagnosis on the basis of clinical history and other noninvasive diagnostic tests. Figure 38.2 depicts a proposed algorithm for the management of pericardial effusion.5 Pericardial tamponade is a Class I indication for pericardiocentesis6 (level of evidence B according to the European Guidelines for the Diagnosis and Management of Pericardial Disease). Pericardiocentesis can also be considered for effusions >20 mm in size on echocardiography and for the diagnosis of smaller effusions when obtaining pericardial fluid is felt to aid in the diagnosis6 (level of evidence B, Class IIa indication; Table 38.1).
Fluoroscopy-Guided Pericardiocentesis
At most centers, pericardiocentesis is performed in the cardiac catheterization laboratory using a combination of echocardiographic and fluoroscopic guidance. It is highly recommended that a two-dimensional echocardiogram be obtained just prior to the procedure to document the presence, location, and size of the effusion; to determine the presence of loculation or significant stranding; and to determine the location on the body surface where the effusion lies closest to the surface and at which the fluid depth overlying the heart is maximal.7 Once an entry location is selected, the echo can indicate the optimal direction for needle passage and the approximate depth of needle insertion that will be required. We believe that in the cardiac catheterization laboratory, access to pressure measurement, continuous ECG and vital sign monitoring, and fluoroscopy with the ability to inject radiographic contrast is highly preferable, particularly in difficult or challenging cases, in patients with small or localized effusions, or when complications ensue. It is important to have access to adequate ancillary support and other technologies in hemodynamically unstable patients, unless an emergency requires a bedside procedure.8 Performing the procedure in the catheterization laboratory in conjunction with right heart pressure measurement is also required if the diagnosis of effusive-constrictive pericarditis is suspected, if the effusion is small or loculated, or if the patient is hemodynamically unstable.
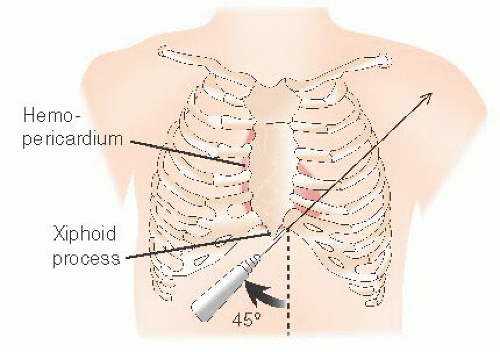
The patient’s torso is propped up to a level of about 45° using a bolster or other mechanism, and the transducers are zeroed to the level of the heart in this position. The subxiphoid approach is classic: a skin nick is made 1 to 2 cm below the costal margin just to the left of the xiphoid process, to allow the needle to miss the ribs. The desired needle path is generally toward the posterior aspect of the left shoulder, passing anterior to or through the anterior capsule of the liver, and entering the pericardial space overlying the right ventricle (Figure 38.3). Echocardiography from the subxiphoid window is thus very useful to confirm the optimal direction toward the pericardial entry point and the approximate depth below the skin. When this geometry is unfavorable—as in posterior effusions or patients with large body habitus—apical or low parasternal intercostal puncture sites are potential alternatives. Since echocardiography does not image through air (and to avoid pneumothorax), sites with significant intervening lung should be excluded; care should be taken in the parasternal approach to avoid the internal mammary artery that runs 3 to 5 cm from the parasternal border, and also the neurovascular bundle at the lower margin of each rib.
Figure 38.2 Management of pericardial effusion. (Reproduced with permission from: Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial disease. Circulation 2010;121:916-928.)
Table 38.1 Utility of Diagnostic Tests for the Etiologic Diagnosis of Pericarditis According to Targeted Causes
Test
General
Tuberculous
Systemic Disease
Neoplastic
Purulent
Auscultation
+++
+/−
+/−
+/−
+/−
ECG
+++
+/−
+/−
+/−
+/−
Echocardiography
+++
+++
++
+++
+++
Markers of inflammation
+++
+++
+++
+++
+++
Markers of myocardial lesion
+++
+/−
+
+/−
+/−
Tumor markers
−
−
+/−
+
−
Tuberculin skin test
−
+/−
+/−
−
−
QuantiFERON-TB
−
+
+/−
−
−
ANA, ENA (anti-SSA)
−
−
+
−
−
HIV testing
−
+
+
−
+
Viral serology
−
−
−
−
−
Blood culture
−
−
−
−
+
Chest x-ray
++
+++
+++
+++
++
CT
−
+++
+++
+++
+++
CMR
−
++
++
+++
+++
Mammography
−
−
−
+++
−
Pericardiocentesis
−
+++
+/−
+++
+++
Pericardial biopsy
−
+++
+/−
+++
+
ANA, antinuclear antibody; CT, computed tomography; CMR, cardiac magnetic resonance; ENA, antibodies anti-extractable nuclear antigen; SSA, Sjogren Syndrome type A; +++, very high; ++, high/good; +, discrete; +/−, low/insufficient; and −, not useful. QuantiFERON-TB is an interferon-γ release assay used in tuberculosis diagnosis.
(Reproduced with permission from Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial disease. Circulation 2010;121:916-928.)
Figure 38.3 Schematic representation of the standard subxiphoid approach for pericardiocentesis. The procedure is usually performed by inserting a thin-walled 18-gauge or a 20-gauge spinal needle below the xiphoid process at a 45-degree angle toward the left shoulder. (From Fleisher GR, Ludwig S, Baskin MN. Atlas of Pediatric Emergency Medicine. Philadelphia: Lippincott Williams & Wilkins, 2004.)
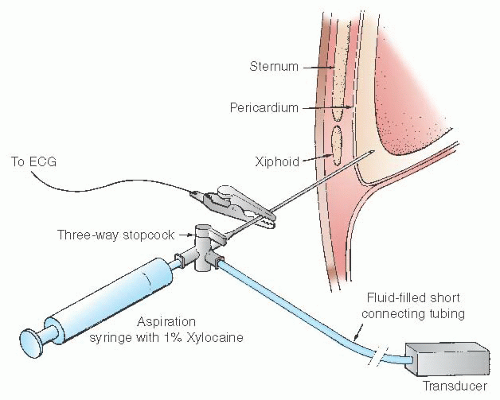
After a sterile prep and appropriate draping, the skin and subcutaneous tissues are infiltrated with lidocaine with a small-gauge needle along the proposed path of entry. We then usually use a 5 to 8 cm, 18 gauge needle attached to a 10 mL syringe filled with saline or lidocaine, which is inserted following the echo-determined trajectory. As the needle is advanced, the syringe is alternately aspirated to determine pericardial space entry and injected to deliver more local anesthesia along the route. If a three-way stopcock is interposed between the syringe and the needle, it can be used to connect to a pressure manifold via a fluid-filled extension tube. Classically, electrocardiographic monitoring of the needle (by attaching its shaft to the V lead of the ECG system using a sterile alligator clip) can be used to provide an additional measure of safety (Figure 38.4): the ST segment recorded from the needle should be isoelectric during advancement, but dramatic elevation of the ST segment appears if the needle contacts the right ventricular epicardium. The needle must be withdrawn slightly until ST elevation resolves, to minimize the chance of right ventricular puncture or laceration. Use of a properly grounded ECG system is imperative to avoid introducing leakage currents through the needle. With the use of fluoroscopy and the ability to inject radiographic contrast and monitor pressure to confirm entry into the pericardial space, most operators no longer use ST segment monitoring during fluoroscopy-guided pericardiocentesis. Importantly, it should be emphasized that ST segment monitoring alone is inadequate as a safeguard from complications.6 A blunt-tip epicardial needle (Tuohy-17) can also be used to minimize risk of right ventricular puncture. This technique may be modified to enable access to the normal pericardium for drug delivery and epicardial mapping (see below).
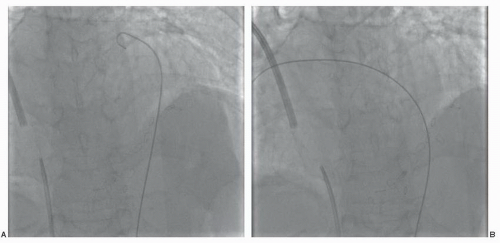
When the needle enters the pericardial space, a distinct pop is usually felt and it is possible to aspirate fluid. If there is an interposed stopcock connected to a pressure transducer, turning the stopcock will allow display of intrapericardial pressure, which should be superimposable on the simultaneously displayed right atrial pressure from the right heart catheter. The waveform should emphatically not resemble that of right ventricular pressure. If the pericardial needle tip displays a right ventricular waveform, the tip is quickly but smoothly withdrawn under continuous hemodynamic monitoring until the overlying pericardial space is entered. Entry into the pericardial space can be confirmed by injection of radiographic contrast or agitated saline echo contrast, or the advancement of a 0.035 inch J wire in the characteristic path wrapping around the heart (Figure 38.5A,B). An 8F dilator is then introduced over the guidewire, followed by a drainage catheter (straight or pig-tail shaped, with multiple side holes) (Figure 38.6). If difficulty is encountered in advancing the drainage catheter, the dilator can be reintroduced and used to substitute an extra-stiff J wire for better support. We usually attach a 50 mL syringe and a three-way stopcock to the drainage catheter, connecting an extension tube from the other port of the three-way stopcock to a drainage bag or vacuum bottle. This allows fluid to be aspirated into the syringe and transferred to the bottle. Removal of as little as 50 mL of fluid is often sufficient to relieve frank tamponade and improve hemodynamics. After removal of 100 to 200 mL of fluid, it is informative to remeasure the pericardial and right atrial pressures before resuming aspiration. Resolution of tamponade physiology usually occurs after aspiration of 50 to 200 mL of fluid. It is recommended that pericardial fluid be removed slowly, as rapid removal can precipitate the development of acute postprocedure ventricular dysfunction9 (see “Complications” below). Occasionally, patients will experience pericardial pain when the effusion is tapped dry. In this case, parenteral narcotic analgesics and benzodiazepines can be administered, and if the pain is severe, 50 mL of pericardial fluid, sterile saline, or 10 to 20 mL of 1% Xylocaine can be reintroduced to help ease the pain. The patient should be laid flat and a final set of pericardial and right heart pressures measured. A fall in pericardial pressure to a level ≤0 mmHg and separation from the right atrial pressure, with a return of the normal diastolic y descent, indicate relief of tamponade physiology. These changes will be accompanied by a resolution of pulsus paradoxus. In previously hypotensive patients, systemic arterial pressure usually rises in association with an increase in mixed venous oxygen content, indicative of an increase in cardiac output. Failure of pericardial pressure to fall close to 0 mmHg indicates that the reference height of the transducers is incorrect or that free or loculated pericardial fluid is still under pressure. If the pericardial pressure falls appropriately but the right atrial pressures remain elevated with prominent x and y descents, the diagnosis of effusive-constrictive pericarditis must be entertained, with an ongoing element of constriction after the tamponade physiology has been relieved (see chapter 23).
Figure 38.4 Diagram showing the subxiphoid approach to pericardiocentesis with pressure and ST segment monitoring. A hollow, thin-walled, 18-gauge needle is connected via a three-way stopcock to an aspiration syringe filled with 1% Xylocaine and to a short length of fluid-filled tubing connected to a pressure transducer. A sterile V lead of an electrocardiographic recorder may be attached to the metal needle hub. The needle is advanced until pericardial fluid is aspirated or an injury current appears on the V-lead electrocardiographic recording. Once fluid is aspirated, the stopcock is turned so that needle-tip pressure is displayed against simultaneously measured right atrial pressure from a right heart catheter. When needle-tip position within the pericardial space is confirmed, a J-tipped guidewire is passed through the needle into the pericardial space, the needle is removed, and a catheter with end and side holes is advanced over the guidewire and subsequently connected via the three-way stopcock to both the transducer and the syringe. This permits, first, thorough drainage of the pericardial effusion using a catheter rather than a sharp needle and, second, documentation that tamponade physiology is relieved when right atrial pressure falls and intrapericardial pressure is restored to a level at or below zero.
Figure 38.5 A, B. Guidewire advanced in the pericardial space with its characteristic path wrapping around the heart.
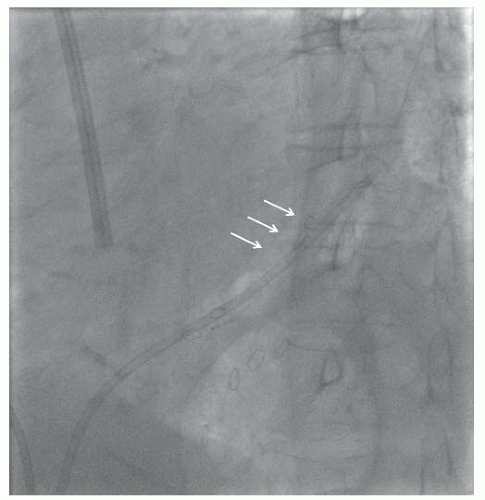
Figure 38.6 Pericardial drain in the pericardial space. The cardiac silhouette and its relation with the catheter are shown by the arrows.
The drainage catheter is then sewn in place and attached to a sterile fluid path (stopcock, syringe, and drainage bag) to allow the postprocedure nursing staff to periodically attempt additional aspiration. Sterility must be strictly maintained with this technique, because regularly interrupting the integrity of the drainage circuit may introduce infectious agents. Some institutions rely on continuous or intermittent suction applied via a water-seal device. The pericardial catheter is removed when the drainage has decreased to <25 to 50 mL per 24 hours and there is no echocardiographic evidence of reaccumulation of fluid. Subsequently, periodic echo reassessment for fluid reaccumulation should be performed. Larger effusions may benefit from slightly more prolonged drainage, but >48-hour dwell time should be avoided to reduce the risk of infection.10 Analysis of pericardial fluid can aid in the diagnosis of infectious pericarditis (fungal, bacterial, viral, and tuberculous), as well as in the diagnosis of malignant and cholesterol effusions.6Table 38.2 summarizes recommended diagnostic tests to be performed on pericardial fluid, as indicated.
Echocardiography-Guided Pericardiocentesis
When performing pericardiocentesis, the ideal entry site would be the point at which the distance from skin to maximal fluid accumulation is minimal, with no intervening vital organs. Echocardiographic guidance has emerged as a technique to identify the ideal entry site and to perform pericardiocentesis safely without fluoroscopy. In a large series of 1,127 patients managed with echocardiography-guided pericardiocentesis, the chest wall entry site was the most commonly used site (79% of patients).4 Importantly, the para-apical approach was used in 80% of patients managed with chest wall entry (714/890), while the remaining chest wall entry sites included the left and right parasternal, left axillary, and posterolateral regions. The pericardial space can be entered using a 16 to 18 gauge polytef-sheathed needle or a similar angiocatheter. Injection of agitated saline through the sheath can be used to confirm position of the sheath in the pericardial space (Figure 38.7), particularly when the needle aspirate is hemorrhagic. In emergency situations, echocardiography-guided pericardiocentesis can be performed at the bedside.
Table 38.2 Diagnostic Tests of Pericardial Fluid
Suspected Malignant Effusion
Cytology and tumor markers (carcinoembryonic antigen—CEA), alphafetoprotein (AFP), carbohydrate antigens (CA 125, CA 72-4, CA 15-3, CA 19-9, CD-30, CD-25, etc.). Differentiation of tuberculous and neoplastic effusion is virtually absolute with low levels of adenosine deaminase (ADA) and high levels of CEA.
Suspected Tuberculosis
Acid-fast bacilli staining; mycobacterium culture or radiometric growth detection (e.g., BACTEC-460); adenosine deaminase (ADA), interferon (IFN)-gamma, pericardial lysozyme, and PCR analyses for tuberculosis (level of evidence B, indication I). Very high ADA levels have prognostic value for pericardial constriction. PCR analysis is as sensitive (75% versus 83%), but more specific (100% versus 78%) than ADA estimation for tuberculous pericarditis.
Suspected Bacterial Infection
At least three cultures of pericardial fluid for aerobes and anaerobes as well as blood cultures are mandatory (level of evidence B, indication I). Gram stains in pericardial fluid have a specificity of 99%, but a sensitivity of only 38% for exclusion of infection.
Viral Infections
PCR analyses for cardiotropic viruses discriminate viral from autoreactive pericarditis (indication IIa, level of evidence B).
Nonspecific Tests
Specific gravity (>1,015), protein level (>3.0 g/dL; fluid/serum ratio >0.5), LDH (>200 mg/dL; serum/fluid ratio >0.6), and glucose (exudates versus transudates: 77.9 ± 41.9 versus 96.1 ± 50.7 mg/dL) can separate exudates from transudates but are not directly diagnostic (class IIb). However, purulent effusions with positive cultures have significantly lower fluid glucose levels (47.3 ± 25.3 versus 102.5 ± 35.6 mg/dL) and fluid-to-serum ratios (0.28 ± 0.14 versus 0.84 ± 0.23) than those of noninfectious effusions.
Cell Counts
White cell count (WBC) is highest in inflammatory diseases, particularly of bacterial and rheumatologic origin. Very low WBC count found in myxedema. Monocyte count is highest in malignant effusions and hypothyroidisms (79 ± 27% and 74 ± 26%), while rheumatoid and bacterial effusions have the highest proportions of neutrophils (78 ± 20% and 69 ± 23%).
Cholesterol Levels
As compared with controls, both bacterial and malignant pericardial fluids have higher cholesterol levels (49 ± 18 versus 121 ± 20 and 117 ± 33 mg/dL).
Epithelial Membrane Antigen, CEA, Vimentin
Combination of epithelial membrane antigen, CEA, and vimentin immunocytochemical staining can be useful to distinguish reactive mesothelial and adenocarcinoma cells.
(Adapted from Maisch B, Seferovic PM, Ristic AD, et al. Guidelines on the diagnosis and management of pericardial diseases: executive summary; the task force on the diagnosis and management of pericardial diseases of the European Society of Cardiology. Eur Heart J 2004;25:587-610.)
Only gold members can continue reading. Log In or Register to continue
Jun 26, 2016 | Posted by drzezo in CARDIOLOGY | Comments Off on Pericardial Interventions: Pericardiocentesis, Balloon Pericardiotomy, and Epicardial Approach to Cardiac Procedures