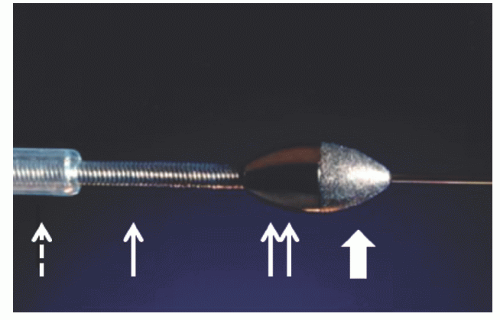
 Figure 29.1 Rotablator burr, drive shaft, and sheath. Ablative distal burr surface (thick white arrow); burr proximal nonablative surface (double arrow); drive shaft (solid white arrow); and Teflon sheath (dashed arrow). (Courtesy of Boston Scientific.) |
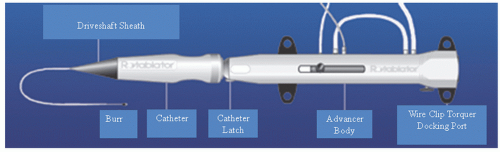 Figure 29.2 Rotalink® advancer. (Courtesy of Boston Scientific.) |
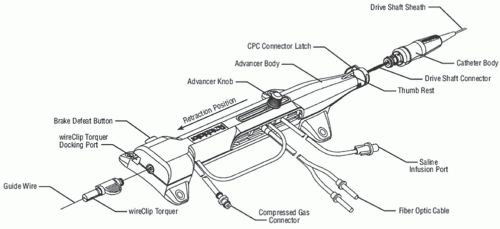 Figure 29.3 Rotalink® advancer. (Courtesy of Boston Scientific.) |
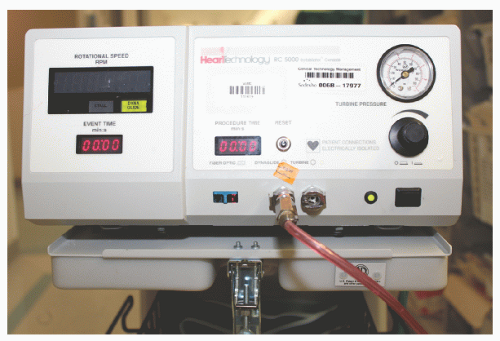 Figure 29.4 Rotablator console front view. Tachometer is in the black window on the left front of the console to display live rotational speed. Illuminated green box will appear when the fixed lower speed dynaglide is activated for burr removal from the body. Duration of individual burr runs and total burr time are displayed in red color in two separate boxes on the console face. On the center bottom of the console face are outputs for fiberoptic cables and for compressed gas lines that will connect to the Rotalink® advancer and the foot pedal. Black control knob on the right front allows adjustment of rotational speed. Turbine pressure is displayed in the dial in upper right corner of the console face. |
This should not be used in patients who are allergic to egg products or olive oil. Various combinations of vasodilators are often added as well to counteract vasospasm and microvascular no-reflow. Typical “RotaFlush” solutions mix 4 mg of nitroglycerin and 5 mg of verapamil in 500 mL of saline. A temporary pacing wire is generally utilized in PTRA of the right coronary or dominant circumflex owing to the risk of profound bradycardia, which is believed to result from adenosine release with red cell fragmentation.
 Figure 29.5 Rotablator console rear view with attached compressed gas tank. |
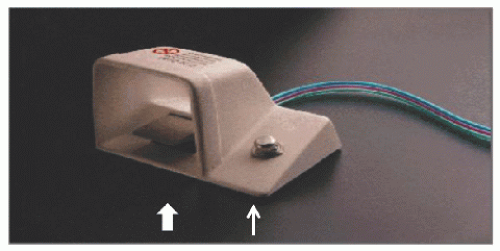 Figure 29.6 Rotablator foot pedal. Foot pedal used to activate the burr (thick white arrow). Dynaglide mode is activated and deactivated using the knob on the right of the foot pedal (thin white arrow). (Courtesy of Boston Scientific.) |
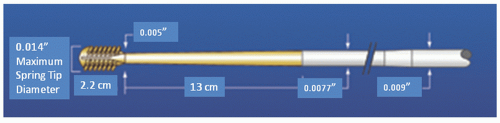 Figure 29.7 Rotablator wires. (Courtesy of Boston Scientific.) |
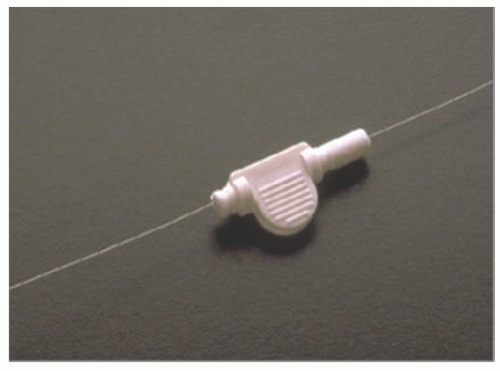 Figure 29.8 Rotablator wire clip. (Courtesy of Boston Scientific.) |
compression in the drive shaft that might otherwise cause the burr to lurch forward into the lesion on activation. Under fluoroscopy, the burr is then activated by the foot pedal and adjusted to the desired “platform” speed (generally 160,000 to 180,000 rpm for burrs ≤2.0 mm, 140,000 to 160,000 rpm for burrs >2.0 mm) before engaging the lesion. Advancement of the lever then brings the spinning burr slowly into contact with the lesion. It is important to be aware of the sound of the turbine, the rotational speed display, and tactile feedback during rotablation. When the burr face encounters excessive resistance to rotation, the speed will fall, but it is essential to avoid speed drops of >5,000 rpm during advancement.8 Larger speed drops caused by excessive pressure on the burr against the lesion may result in the liberation of larger particles, frictional heating of the plaque, or torsional dissection. We prefer advancing with a “pecking” motion in which brief (1 to 3 seconds) periods of plaque contact are alternated with longer (3 to 5 seconds) periods of reperfusion provided by pulling the burr back from the plaque face. This reduces speed drops and aids in the clearance of particulate debris through the distal circulation. Some operators favor intermittent injections of dilute contrast through the guide during the burr run to monitor for vessel complications and to enhance clearance of particulate debris.
calcified lesions.20, 21, 22 In a single-center series, PTRA followed by drug-eluting stenting (DES) for calcified lesions was associated with reduced target lesion revascularization rates as compared to PTRA plus bare-metal stenting (BMS) (10.6% versus 25%, P < 0.001).23 Another single-center series has suggested that when PTRA is utilized to deliver and expand DES in heavily calcified lesions, clinical outcomes are similar to those of DES alone.24 However, no study has demonstrated superiority of PTRA plus DES over DES alone, even in calcified lesions. Current PCI guidelines provide a Class IIa recommendation for PTRA in heavily calcified or fibrotic lesions that may not dilate with conventional techniques prior to stenting.13
Table 29.1 Randomized Clinical Trials of Percutaneous Transluminal Rotational Atherectomy | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
of DES. Heavily calcified lesions are the most common indication for PTRA. An illustrative example of the utility of PTRA is presented in Figures 29.9, 29.10, 29.11, 29.12, 29.13, 29.14, 29.15, 29.16, 29.17 and 29.18. Rotablator should be avoided if there is angiographic evidence of dissection, thrombus, slow flow or no-reflow (Figure 29.17), excessive vessel tortuosity, or severe left ventricular dysfunction. When aggressive balloon angioplasty has failed to dilate a lesion, PTRA at the same setting should only be considered with caution (Figures 29.9, 29.10 and 29.11). If balloon-generated dissection is present, PTRA could compound the dissection or induce perforation. Rotational atherectomy has been used to pass through a stent cell to revascularize an ostial lesion in a jailed side branch. However, it is recommended that this approach be used only if the stent cell has been previously dilated; and a small burr is recommended, given that serious complications have been encountered when the burr could not be retracted through the stent.
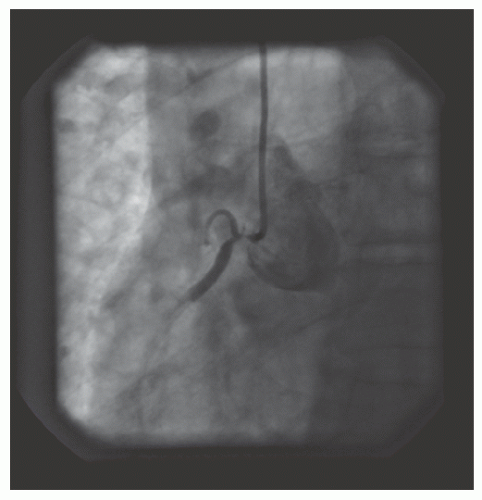 Figure 29.9 Ostial right coronary artery lesion. Modest superior calcification is present, but not well reproduced in this image. Pressure damping occurs with any attempted engagement from a radial approach. |
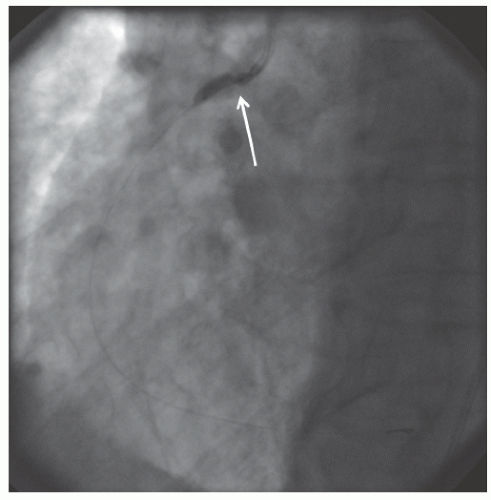 Figure 29.10 Balloon inflation with a 2.5-mm noncompliant balloon at 18 atm shows a severe waist at the ostium (white arrow), consistent with a nondilatable lesion. |
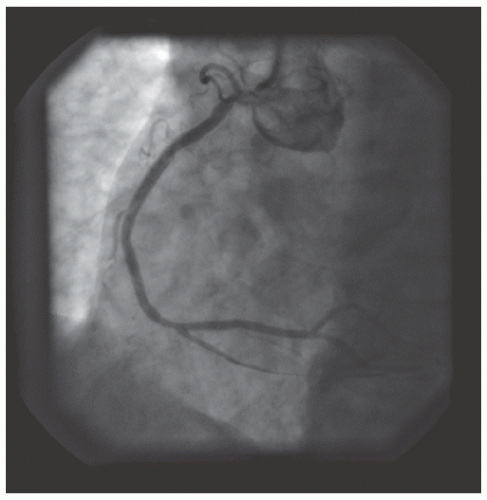 Figure 29.11 Final result after inflation with a 2.5-mm noncompliant balloon at 18 atm. Severe residual stenosis can be seen. |
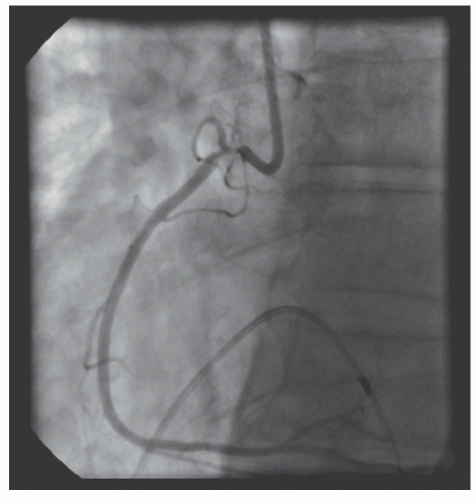 Figure 29.12 Engagement of the right coronary artery with an 8F internal mammary guide from a femoral approach. Severe damping occurs with any engagement. A temporary pacing wire is placed in the right ventricle. |
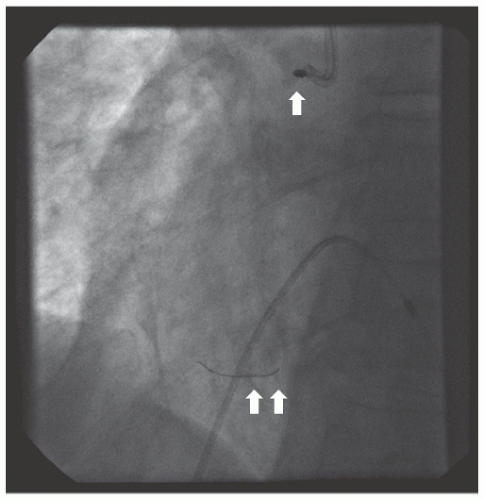 Figure 29.13 Rotablator burr (2.0 mm; white arrow) being advanced over a RotaWire™ floppy wire (white double arrow). Prior to this, the lesion has been treated with 1.25- and 1.5-mm burrs. Temporary pacing wire in the right ventricle. |
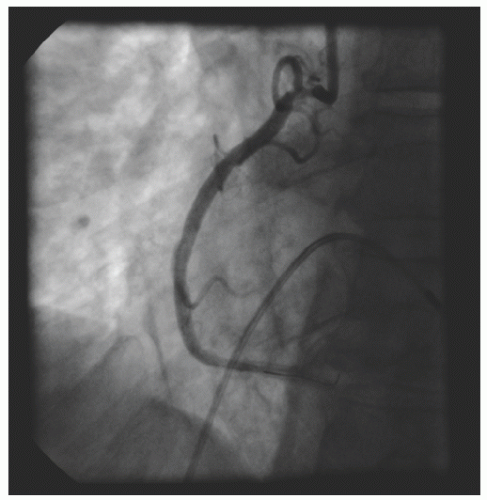 Figure 29.14 Result after 2.0-mm burr. Significant residual stenosis. |
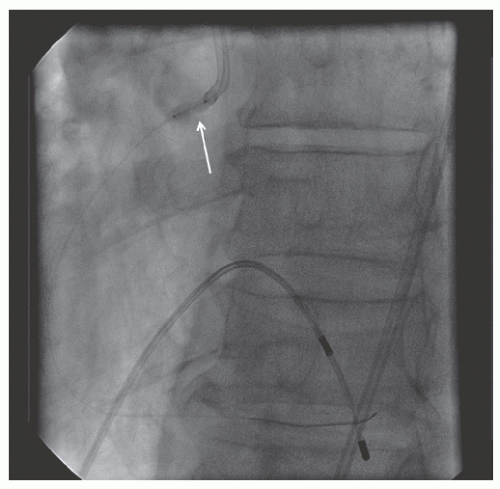 Figure 29.15 Balloon inflation with a noncompliant 3.0-mm balloon after 2.0-mm rotablation still demonstrates persistent waisting (white arrow) of the balloon consistent with an undilatable lesion. |
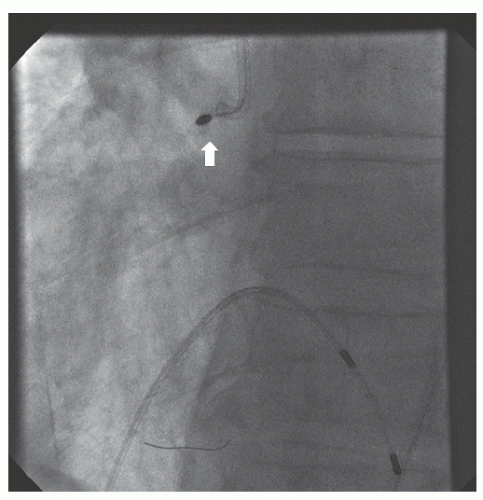 Figure 29.16 Rotablator burr (2.15 mm; white arrow) being advanced over RotaWire™ floppy wire. |
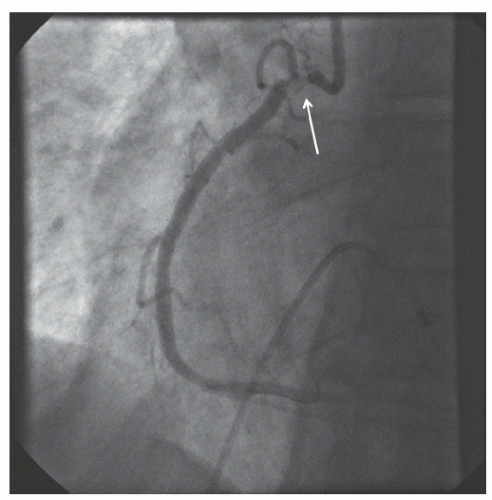 Figure 29.17 Result after 2.15-mm burr. There is some irregularity of the very ostial vessel (white arrow) and there is mild slow flow distally. Rotational atherectomy is stopped at this point due to concerns of precipitating severe no reflow. |
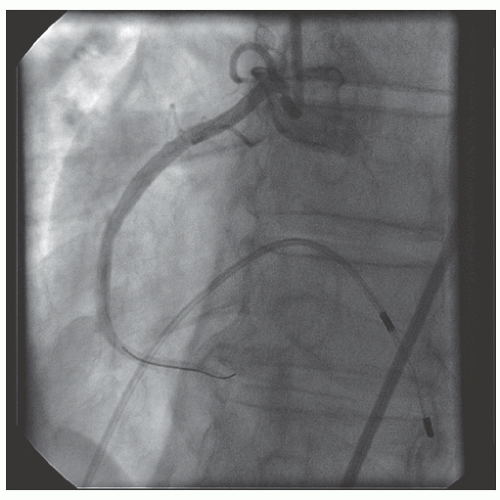 Figure 29.18 Final result after 3.0 mm × 18 mm drug-eluting stent, postdilated to 3.5 mm and then to 4.0 mm at 22 atm at the very ostium. |
at 6 months, however. A strategy of more extensive plaque removal and routine postdilation to achieve a residual diameter stenosis of <20% was tested in the Balloon Angioplasty versus Optimal Atherectomy Trial (BOAT).36 Six months’ angiographic restenosis was reduced with optimal DCA as compared to BA (31.4% versus 39.8%; P = 0.016), but revascularization rates and mortality at 1 year were not reduced. In the Atherectomy before Multi-link Improves Lumen Gain and Clinical Outcomes (AMIGO) study, optimal DCA plus baremetal stenting did not improve restenosis rates or clinical outcomes as compared to bare-metal stenting alone.37 Based on these results and the emergence of DES, DCA is no longer marketed.
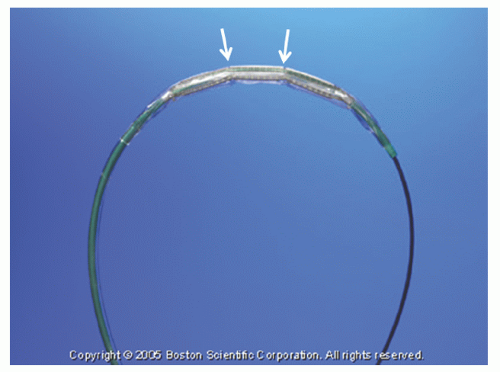 Figure 29.19 Cutting balloon. White arrows indicate flexion points on the atherotomes. (Courtesy of Boston Scientific.) |
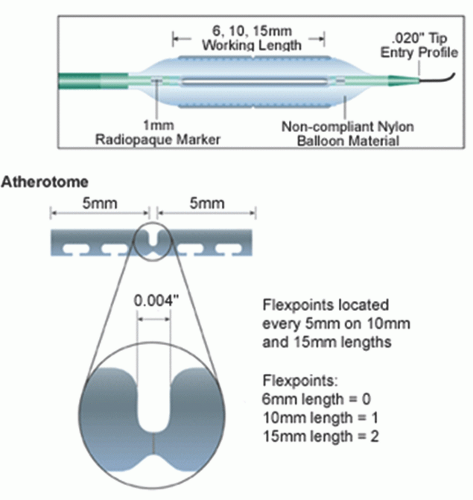 Figure 29.20 Atherotomes and flexion points on cutting balloon. (Courtesy of Boston Scientific.) |
Table 29.2 Cutting Balloon Angioplasty Trials | ||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


