Chapter 43 Nonsustained Ventricular Tachycardia
Nonsustained ventricular tachycardia (NSVT) has been recognized as a usually asymptomatic rhythm disorder detected in an extremely wide range of conditions, from asymptomatic, apparently healthy, young individuals to patients with significant heart disease. Because of its brevity, NSVT does not produce symptoms in most instances; it derives its clinical importance from the fact that its detection may have important prognostic implications, depending on the underlying pathology. In several clinical settings, NSVT is a marker of increased risk for subsequent sustained tachyarrhythmias and sudden cardiac death (SCD), whereas it may have no prognostic significance in a healthy individual, although evidence for occult pathology or an inherited channelopathy in apparently normal subjects who develop ventricular arrhythmia not related to physical exercise continues to accumulate.1–3 The main task of the physician is to detect the apparently healthy individuals in whom NSVT represents a sign of occult disease and to risk stratify patients with known disease who present with this arrhythmia. This, however, is not an easy task. The patient with NSVT still represents a clinical challenge with regard to proper management, and several crucial questions remain unanswered.
Definition
Traditionally, the term tachycardia (from the Greek words tachy, meaning fast, and cardia, meaning heart) is used to describe conditions in which the heart rate exceeds the conventional number of 100 beats/min for more than three consecutive beats, either in response to metabolic demand or other stimuli or because of disease.4 Sustained tachycardia is defined as tachycardia that lasts for more than 30 seconds (unless requiring termination because of hemodynamic collapse), whereas nonsustained tachycardia terminates spontaneously within 30 seconds.4 Thus, NSVT has been defined as three (sometimes five) or more consecutive beats arising below the atrioventricular (AV) node with an R-R interval of less than 600 ms (>100 beats/min) and lasting less than 30 seconds.5
This definition is by no means a universally accepted one. In the recent Cardiac Arrhythmias and Risk Stratification After Acute Myocardial Infarction (CARISMA) study,6 NSVT was detected by registering runs of 16 beats or more, with a rate of 125 beats/min, whereas a rate of 120 beats/min or more has been used by the Marburg trial and other studies.7,8 The period of a tachycardia run to qualify for NSVT has also varied. In the Electrophysiologic Study Versus Electrocardiographic Monitoring (ESVEM) study, the time cut-off was 15 seconds as opposed to the conventional number of 30 seconds, which has been used both by the Multicenter Automatic Defibrillator Implantation Trial (MADIT) and the Multicenter Unsustained Tachycardia Trial (MUSTT) .9–11 This implies that NSVT cases according to the MADIT and MUSTT criteria might well have been dealt with as sustained ventricular tachycardia (VT) episodes in the ESVEM cohort. In other studies, the terms ventricular ectopy or NSVT are often used without strictly defined diagnostic criteria.12
Epidemiology
Reliable epidemiologic data on NSVT are difficult to obtain. Usually, although not invariably, most patients remain asymptomatic, and the reproducibility of NSVT recordings is documented in only half of the patients with this arrhythmia. In the MADIT, NSVT was defined as reproducible when found in at least two recordings of three consecutive Holter electrocardiograms (ECGs) performed in weekly intervals. Reproducible NSVT was identified in only 50% of the patients with NSVT and did not seem to be an independent risk factor for future arrhythmic events.13 The reported prevalence of NSVT in various clinical conditions is presented in Table 43-1. Previous studies were based on Holter monitoring, thus reporting NSVT occurring within a short period. The advent of implantable permanent pacemakers, defibrillators, and monitoring devices with extensive ECG monitoring capabilities has allowed for a more accurate estimation of the incidence of NSVT in patients with heart disease. Evidence is now available from implantable cardioverter-defibrillator (ICD) data that NSVT is a distinct tachyarrhythmia that may cause syncope without causing death in patients with heart disease and that the incidence of polymorphic NSVT relative to sustained arrhythmia is greater than previously believed.14
Table 43-1 Reported Prevalence of Nonsustained Ventricular Tachycardia in Different Cardiac Conditions
| CONDITION | PREVALENCE |
|---|---|
| Apparently healthy individuals | 0%-3% |
| Non-ST ACS (2 to 9 days after admission) | 18%-25% |
| Acute MI (early phase) | 45%-75% |
| Reperfused acute MI (later than 1 week) | 7%-13% |
| Heart failure (LVEF <30% to 40%) | 30%-80% |
| DCM | 40%-50% |
| HCM | 25%-80% |
| Significant valve disease | ≤25% |
| Hypertension | 8% |
| Hypertension and left ventricular hypertrophy | 12%-28% |
DCM, Dilated cardiomyopathy; HCM, hypertrophic cardiomyopathy; LVEF, left ventricular ejection fraction; MI, myocardial infarction; Non-ST ACS, non–ST-segment elevation acute coronary syndrome.
In asymptomatic, apparently healthy persons, Holter recordings in older studies revealed a frequency of NSVT ranging from 0% to 3%.5,15,16 In non–ST-segment elevation acute coronary syndromes, NSVT is detected in 18% to 25% of patients 2 to 9 days after admission.17 In acute myocardial infarction (MI), NSVT during the first 24 hours is frequent (43% in patients without thrombolysis and up to 75% in re-perfused patients).5,18 In the first 7 days after MI, NSVT is detected in approximately 6.8% to 13.4% of patients in the reperfusion era, which is not much different from that reported in the pre-thrombolytic era (12%; Multicenter Postinfarction Research Program).18–23 NSVT can be detected in approximately 2% of patients with ischemia and preserved left ventricular function.24 Recently, the CARISMA study group reported on long-term cardiac arrhythmias recorded by a cardiac monitor implanted 2 to 5 days after MI in patients with left ventricular ejection fraction (LVEF) of 40% or less. The detected incidence of NSVT over a 2-year period was 13%.6
In patients with heart failure and LVEF less than 30% to 40%, the reported prevalence of NSVT is 30% to 80%.25,26 It seems that ischemic heart failure carries a higher risk for NSVT. In the Grupo de Estudio de la Sobrevida en la Insuficiencia Cardiaca en Argentina (GESICA) trial, in which only one third of patients had ischemic heart disease, the prevalence of NSVT was 33%. Whereas in the Congestive Heart Failure: Survival Trial of Antiarrhythmic Therapy (CHF-STAT) trial, in which the ischemic patients comprised two thirds of the whole cohort, the prevalence was 80%.25,26 In dilated cardiomyopathy (DCM), NSVT has been detected in 40% to 50% of patients.27–29 In hypertrophic cardiomyopathy (HCM), 20% to 30% of patients may have NSVT, whereas in patients with a history of cardiac arrest, this proportion approaches 80%.30–32 These estimations may not reflect the true incidence of NSVT in HCM, since they are based on highly selected referral populations. In patients with valvular disease, the incidence of NSVT is considerable (up to 25% in aortic stenosis and in significant mitral regurgitation) and appears to be a marker of underlying left ventricular pathology.33,34 In patients with arterial hypertension, NSVT is correlated to the degree of cardiac hypertrophy and subendocardial fibrosis.35,36 Approximately 12% to 28% of patients with hypertension and left ventricular hypertrophy present with NSVT as opposed to 8% of patients with hypertension alone.35,36 Ventricular extrasystolic activity can be detected with Holter monitoring in up to 50% of patients with repaired tetralogy of Fallot, and recent studies have detected a 4% to 14% prevalence of sustained VT.37–39
Clinical Electrocardiography
Electrocardiographic Patterns
Nonsustained Ventricular Tachycardia Associated with a “Normal” Heart
In the apparently normal population, NSVT episodes without consistent morphology patterns may be recorded either at rest or after exercise. 15,16,40–44 When NSVT is documented in the context of a history of established monomorphic VT, it may demonstrate the same morphology as clinical sustained arrhythmia. VTs with a left bundle branch block (LBBB) pattern and inferior axis originate in the right ventricular outflow tract (RVOT).45 Left ventricular outflow tract (LVOT) tachycardias may produce a right bundle branch block (RBBB) morphology with inferior axis or a variable QRS morphology, depending on the site of origin. Tachycardias originating in the left coronary cusp have a QRS morphology consistent with an M or W pattern in lead V1, tachycardias originating in the right coronary cusp have an LBBB pattern, and those from the aortomitral continuity usually result in a qR pattern.46 Idiopathic left VT may also be caused by re-entry within the Purkinje network and may originate within one of the fascicles of the left bundle branch (fascicular tachycardias), and usually the posterior fascicle is involved, resulting in a tachycardia with RBBB and left-axis deviation. However, cases with an inferior axis, that is, of anterior fascicular origin, have also been described.47,48
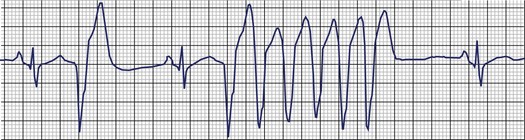
The most systematic attempts to characterize the electrocardiographic pattern of NSVT have been reported to be successful in patients with the so-called repetitive monomorphic VT, originally described by Gallavardin.49 This arrhythmia represents a form of the spectrum of idiopathic ventricular outflow tachycardias, which includes repetitive uniform premature ventricular contractions (PVCs) and exercise-triggered paroxysmal VT. They usually originate in the RVOT and less often in the LVOT and are most probably caused by triggered activity secondary to cyclic adenosine monophosphate–mediated delayed afterdepolarizations.45 The relatively consistent recording of frequent arrhythmia episodes in patients with repetitive monomorphic VT has made possible the accumulation of useful information on its morphology. Holter studies have revealed that the tachycardia begins with a fusion complex or with an ectopic beat that has the same morphology as the subsequent beats (Figure 43-1).50 The salvos of VT are generally short (3 to 15 beats) and the coupling interval of the first beat is usually long (>400 ms). The coupling intervals of successive beats may gradually become prolonged.51–53 Many patients mostly have ventricular premature beats (VPBs) with only occasional episodes of tachycardia, whereas others manifest mainly with short runs of VT, where the tachycardia beats far exceed the number of sinus beats. The rate during tachycardia is generally 110 to 150 beats/min. The arrhythmia is only present within a critical window of heart rates (upper and lower thresholds).50 Thus, the tachycardia often occurs during exercise but disappears as the heart rate increases and returns during the recovery period following exercise. Some patients develop sustained episodes (>30 seconds) during the recovery phase, and this behavior differentiates repetitive monomorphic VT from the exercise-triggered paroxysmal VT first described by Wilson and others in patients with apparently normal hearts.54–56 It should be noted, however, that repetitive behavior has been documented in various clinical settings, including cardiomyopathy and previous MI, as well as tachycardias originating in the aortic valve cusps.51,57

In catecholaminergic polymorphic VT, a familial condition mainly caused by mutations in the genes encoding the cardiac ryanodine receptor channel as well as calsequestrin involved in calcium kinetics, episodes of provoked tachycardia are typically nonsustained.58 They may originate from the LVOT and less frequently from the RVOT or the right ventricular apex. QRS morphology suggests an outflow tract origin of the initiating beat in more than 50% of patients, and subsequent beats portray a polymorphic or typically bi-directional VT morphology.59
Ischemic Heart Disease
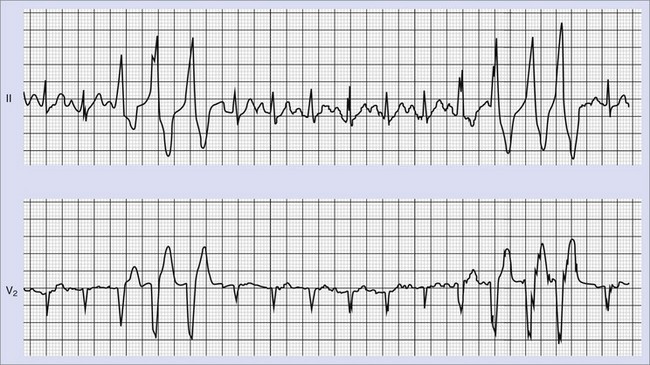
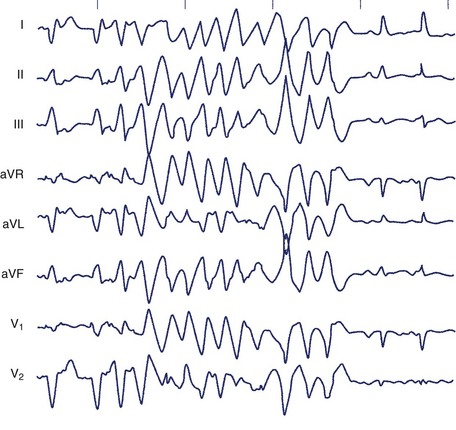
Frequent and complex ventricular ectopy as well as NSVT occur more commonly in patients with left ventricular dysfunction. Usually, monomorphic VT is seen in the context of re-entry at the borders of a ventricular scar caused by previous MI, whereas ischemia most of time induces polymorphic VT or ventricular fibrillation (VF).60,61 The QRS morphology during monomorphic tachycardia may show an RBBB or LBBB pattern or may even be nonspecific (Figure 43-2). Both RBBB and LBBB patterns can be seen in the same patient when the infarct scar involves the interventricular septum (Figure 43-3). Spontaneous reversions to sinus rhythm, thus documenting nonsustained VF, can occur (Figure 43-4), and data from patients with ICDs reveal that up to 40% of all VF episodes are nonsustained.14
Cardiomyopathies and Other Conditions
VTs (both sustained and nonsustained) in DCM may present with multiple morphologies or an LBBB or RBBB pattern. In approximately one third of the cases of idiopathic DCM, and probably in a small percentage of ischemic patients, sustained or nonsustained VT is caused by bundle branch re-entry.62 The necessary condition for bundle branch re-entry seems to be prolonged conduction in the His-Purkinje system, which is reflected in the H-V interval that is prolonged during sinus rhythm and prolonged or equal to the baseline sinus rhythm during VT.63 The circuit involves the right and left branch bundles, with antegrade conduction occurring most of the times through the right branch. As a rule, AV dissociation is present. These tachycardias are usually unstable; the 12-lead ECG, when obtainable, may show an LBBB or RBBB pattern, depending on the orientation of activation of the bundle branches.
No characteristic electrocardiographic morphology of NSVT exists in patients with HCM. Relatively slow, often asymptomatic nonsustained episodes of monomorphic VT may be documented on prolonged ambulatory recordings. When nonsustained or sustained VT is induced by programmed stimulation, it is more often polymorphic (60% of patients) than monomorphic (30%).32,64,65
In other conditions such as valvular disease and systemic hypertension, ventricular arrhythmias are common but less well characterized and usually represent polymorphic rhythms.34–36 Most of the reported patients with mitral valve prolapse demonstrate LBBB morphology during tachycardia, which raises the possibility that the mitral valve prolapse might be an incidental finding or that the arrhythmia is caused by other mechanisms not directly related to the mechanical stress imposed on the ventricle by the valvular apparatus.66,67
The tachycardias in arrhythmogenic right ventricular dysplasia (ARVD) arise from the right ventricle and typically present with LBBB morphology with a left- or even right-axis deviation.68
Long QT Syndrome
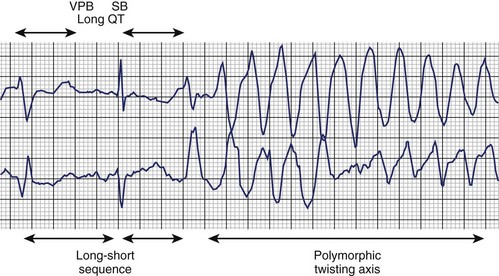
The typical morphology of recorded arrhythmias in long QT syndrome (LQTS; congenital or acquired) is that of torsades de pointes.69 The term refers to the electrocardiographic appearance of spike-like QRS complexes that rotate irregularly around the isoelectric line at rates of 200 to 250 beats/min (Figure 43-5). Typically, the coupling interval of the initial beat of the torsade is long (600 to 800 ms), whereas the last QRS complex of the episode is larger than the normal QRS during sinus rhythm. This is a VT that is frequently nonsustained and sometimes sustained. The tachycardia, which usually occurs in the setting of bradycardia or long postectopic pauses, is often repetitive and may trigger VF. It is seen primarily in association with prolongation of the Q-T interval that may be appreciable before the onset of arrhythmias or after a pause. Not all patients with the LQTS have polymorphic VT with a characteristic torsades de pointes configuration, and this pattern can be seen in some patients without the LQTS. A variety of torsade initiating with a short coupling interval in patients without any evidence of LQTS has also been described.70
Clinical Evaluation
Trans-thoracic Echocardiography
Trans-thoracic echocardiography may detect signs of cardiomyopathy, ARVD and other structural abnormalities, and impaired left ventricular function. Overwhelming evidence indicates that in patients with heart disease, in general, LVEF is the major determinant of cardiac and total mortality.1 The results of the MADIT, MUSTT, Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT), and the Marburg Cardiomyopathy Study (MACAS) trials have also established the importance of LVEF as the most critical prognostic factor in patients with ischemic heart disease and NSVT.8,10,11,71 Left ventricular function assessment with echocardiography or radionuclide ventriculography is therefore mandatory for the risk stratification and subsequent management of patients with NSVT. However, LVEF does not always predict ICD intervention in patients with ischemic or nonischemic cardiomyopathy.72 Analysis of arrhythmic death in 674 patients enrolled in MUSTT showed that patients whose only factor is ejection fraction (EF) of 30% or less have a predicted 2-year arrhythmic death risk of 5% or less.73 Multiple additional factors influence arrhythmic death in patients with LVEF less than 40% and NSVT such as inducible VT, history of heart failure, NSVT not discovered within 10 days after coronary artery bypass grafting (CABG), and intraventricular conduction delay or LBBB.73
Tests for Myocardial Ischemia
Functional tests such as treadmill exercise electrocardiography, myocardial perfusion, and stress echocardiography are required to demonstrate myocardial ischemia in patients with NSVT. Acute myocardial ischemia is an established cause of polymorphic ventricular rhythms.61 The association of monomorphic VT, a substrate-dependent arrhythmia, with acute ischemia is less well characterized, but ischemia may induce monomorphic VT in the presence of a myocardial scar.74–76
Apart from demonstration of ischemia, exercise tasting may also be helpful in patients with LQTS, exercise-triggered RVOT tachycardia, and cathecholaminergic polymorphic VT. NSVT induced by treadmill exercise testing aimed at evaluating presumed LQTS suggests catecholaminergic polymorphic VT rather than LQTS.77
Ambulatory Electrocardiographic Monitoring
Holter monitoring is a valuable diagnostic tool in detecting patients with NSVT, and 7-day Holter monitoring improves detection and allows better characterization of ventricular arrhythmic episodes.78 Detection of NSVT has been reported to predict SCD in patients with non–ST-segment elevation acute coronary syndromes, thrombolysed MI, DCM, HCM, and arrhythmogenic right ventricular dysplasia.17,18,25,31,79–81 However, whether NSVT provokes arrhythmia or is simply a surrogate marker of a more severe underlying cardiac condition is not known. In patients with revascularization of most infarct-related arteries (78%), NSVT early after MI (4 to 16 days) carried a significant but low RR for the composite endpoint of cardiac death, VT, or VF but not for arrhythmic events considered alone.20 In the Danish Multicenter Randomized Study on Thrombolytic Therapy Versus Acute Coronary Angioplasty in Acute Myocardial Infarction-2 (DANAMI-2) trial, the prognostic value of NSVT was limited regardless of reperfusion strategy, and in the study of Makikallio et al, no Holter variable predicted sudden death among infarct survivors with an LVEF of 35% or less.22,79 It seems that in the β-blocking era, all common arrhythmia risk variables, including NSVT, have diminished the predictive power in identifying patients with previous MI at risk of SCD.82
Both in MACAS and CHF-STAT, in patients with CM or ischemic cardiomyopathy, NSVT was a predictor of arrhythmia in univariate analysis but not in multivariate analysis, as opposed to LVEF.8,26 In patients with HCM, NSVT was associated with SCD, but a relation between the risk of arrhythmic death and the frequency, duration, and rate of NSVT episodes could not be demonstrated.31
The suppression of frequent ventricular ectopy or NSVT runs following β-blockade or amiodarone therapy does not imply a favorable diagnosis. Mortality was increased in the Cardiac Arrhythmia Suppression Trials (CAST and CAST II) despite reduced ectopic activity, whereas mortality was not reduced by amiodarone in the Veterans Administration CHF-STAT despite the elimination of ventricular ectopy.83–85 Thus, Holter monitoring may be useful for risk stratification purposes by means of detecting episodes of NSVT in certain clinical settings, but its use for the subsequent follow-up and evaluation of treatment is limited.
Assessment of Autonomic Tone
Heart rate variability (HRV) has been used as an independent risk factor for cardiac mortality in patients with previous MI and has been claimed to be a specific predictor of arrhythmic rather than total cardiac mortality.86–88 In these patients, a depressed baroreflex sensitivity has been associated with increased cardiac mortality and SCD and with a higher predictive power (in values below 3 ms/mm Hg) compared with LVEF, signal-averaged ECG (SAECG), or HRV.89,90 Analysis of patients in the Autonomic Tone and Reflexes After Myocardial Infarction (ATRAMI) trial has shown that NSVT, HRV, and depressed baroreflex sensitivity were all significantly and independently associated with increased mortality. Depressed baroreflex sensitivity, in particular, identified a subgroup with the same mortality risk as patients with NSVT and reduced LVEF.21
However, the Multiple Risk Factor Analysis Trial (MRFAT) show that in the β-blocking era, the common arrhythmia risk variables, particularly the autonomic and standard ECG markers, have limited predictive power in identifying patients at risk of SCD.82 In 43 ± 15 months of follow-up in 675 patients, SCD was weakly predicted only by reduced LVEF (<40%), NSVT, and abnormal SAECG but not by autonomic markers or ECG variables. The positive predictive accuracy of these markers (low LVEF, NSVT, and abnormal SAECG), however, was low at 8%, 12%, and 13%, respectively.82 The smaller Bucindolo Evaluation in Acute Myocardial Infarction Trial (BEAT) study also refuted the predictive value of HRV, the prognostic information of which was found to be contained completely in heart rate.91 In patients with nonischemic cardiomyopathy, results on the value of HRV have been conflicting.7,92,93 Heart rate turbulence and deceleration capacity are newer noninvasive measures of cardiac autonomic regulation that are currently under study.94 More data are clearly needed to establish the clinical usefulness of autonomic markers, particularly in the setting of NSVT.
Signal-Averaged Electrocardiography
The clinical value of SAECG in patients with NSVT by means of determining prognosis and identifying patients in need for an aggressive antiarrhythmic management has not been established yet. In patients presenting with unexplained syncope, the presence of late potentials is a good predictor of induction of sustained VT, and in survivors of MI an abnormal SAECG has been associated with increased risk of arrhythmic and total mortality.95–98 However, its positive predictive value in this setting is low (<30%) as opposed to its high negative predictive value (90%). Thus, a negative SAECG might obviate the need for further investigations when the suspicion of a ventricular arrhythmia is low, but in the case of a high suspicion of ventricular arrhythmia, a negative SAECG is not sufficient evidence for the exclusion of sustained VT or NSVT as the cause of syncope. Furthermore, in patients treated with thrombolysis or β-blockers, the predictive ability of SAECG is limited.82,99 In patients with DCM, SAECG does not predict SCD, but in arrhythmogenic right ventricular dysplasia, SAECG can identify those with more extensive disease and a propensity for inducible VT at programmed electrical stimulation, and is now considered a minor diagnostic criterion.8,81,100
T-Wave Alternans
T-wave alternans (TWA) is a test that is thought to reflect dispersion of repolarization and has been shown to predict VT inducibility and future arrhythmic events better than SAECG.101 In patients similar to those in MADIT II, a microvolt TWA (MTWA) test was found to be better than QRS duration at identifying high-risk patients as well as patients unlikely to benefit from ICD therapy.102 Recently, in patients with reduced LV function (LVEF <40%) and NSVT, MTWA also predicted unstable ventricular tachyarrhythmias better than electrophysiology testing and LVEF less than 30%.103 However, in a later study, although TWA predicted higher total mortality in a MADIT II–like population, the risk of tachyarrhythmic events did not differ according to TWA results.104 The Alternans Before Cardioverter Defibrillator (ABCD) study was the first trial to use MTWA to guide prophylactic ICD insertion in patients with LVEF less than 40% and NSVT. Risk stratification strategies using noninvasive MTWA versus invasive electrophysiological study (EPS) were comparable at 1 year, with very low positive predictive values and very high negative predictive values and complementary when applied in combination. Strategies that use MTWA, EPS, or both might identify subsets of patients least likely to benefit from ICD insertion.105
Electrophysiology Testing
Induction of sustained arrhythmia by programmed electrical stimulationstill retains a predictive power in patients with ischemia who have impaired left ventricular function. According to a meta-analysis, in patients with ischemia and NSVT, the induction of sustained VT is associated with a two- to three-fold increased risk of arrhythmia-related death in a previous meta-analysis.106 In NSVT, in the context of reduced LVEF (<40%), inducibility of sustained monomorphic VT at baseline programmed electrical stimulation was associated with a 2-year actuarial risk of SCD or cardiac arrest of 50% compared with a 6% risk in patients without inducible VT.107 Analysis of patients enrolled in the MUSTT as well as of those in the registry revealed that noninducible patients have a significantly lower risk of cardiac arrest or SCD compared with inducible patients at 2 and 5 years (12% vs. 24% and 18% vs. 32%, respectively).108 Still, however, as these results indicate, patients with noninducible sustained VT are not free of risk of SCD. The MUSTT investigators have further analyzed the relation of EF and inducible ventricular tachyarrhythmias to mode of death in 1791 patients who were enrolled in MUSTT and did not receive antiarrhythmic therapy. Total and arrhythmic mortality were higher in patients with an EF less than 30% than in those whose EFs were 30% to 40%. The relative contribution of arrhythmic events to total mortality was significantly higher in patients with inducible tachyarrhythmia (58% of deaths in inducible patients vs. 46% in noninducible patients; P = .004). The higher percentage of events that were arrhythmic among patients with inducible tachyarrhythmia appeared more distinct among patients with an EF of 30% or greater (61% of events were arrhythmic among inducible patients with an EF ≥30% and only 42% among noninducible patients; P = .002). This study therefore suggested that the major usefulness of EPS may be restricted to patients having an EF between 30% and 40%.109 The prognostic significance of VT inducibility appears to be similar to that of VT induced by one, two, or three extrastimuli.110 These results should be considered in the context of evidence from analysis of stored ICD data that has shown that little association exists between spontaneous and induced ventricular arrhythmias.111
The role of programmed electrical stimulation has not been established in the patient with ischemia and relatively preserved left ventricular function (LVEF >40%), although some evidence indicates that inducibility of sustained VT or VF at programmed electrical stimulation might retain discriminative ability by means of identifying a higher risk patient cohort.112,113 The prognostic usefulness of programmed stimulation in patients with nonischemic DCM, including those with NSVT, remains controversial.114–116 Retrospective cohort analysis of 54 patients from the Mayo Clinic showed that programmed electrical stimulation did not differentiate patients with and those without appropriate ICD shocks.114 However, inducibility of polymorphic VT or VF is a much stronger predictor of recurrences of fast VT as opposed to sustained monomorphic VT induction in DCM patients with ICD for secondary prevention.117 Daubert et al, in the Defibrillators in Non-Ischemic Cardiomyopathy Treatment Evaluation (DEFINITE) trial, reported that inducibility tested via ICD was found in 29 of 204 patients (VT in 13, VF in 16) and that at follow-up, 34.5% of the inducible group (10 of 29) had ICD therapy for VT or VF or arrhythmic death versus 12% (21 of 175) of noninducible patients (hazard ratio [HR], 2.60; P = .014).118 Thus, inducibility of ventricular arrhythmias, especially polymorphic VT or VF, indicates increased likelihood of subsequent ICD therapies and might be considered a useful risk stratifier.
Programmed ventricular stimulation is of diagnostic as well as prognostic value in risk stratifying patients with repaired tetralogy of Fallot.119 In multivariate analysis of a study on 252 patients with repaired tetralogy, inducible sustained monomorphic or polymorphic VT was an independent risk factor for subsequent events (RR, 4.7; 95% confidence interval [CI], 1.2–18.5; P < .0268).119
Little evidence exists for benefit from EPS in patients with HCM and NSVT. In patients with a history of cardiac arrest, polymorphic VT that deteriorates into VF was induced in approximately half only.32,64,65
Cardiac Magnetic Resonance Imaging
In patients with previous MI, necrotic myocardium and viable myocardium coexisting within the same wall segments, as detected by delayed enhancement cardiac magnetic resonance imaging (CMRI), predicts the occurrence of NSVT in patients without left ventricular dilation, whereas left ventricular mass and end-systolic volume are predictors of NSVT in those with left ventricular dilation.120 In patients with HCM, the presence of delayed enhancement on contrast-enhanced CMRI is associated with increased likelihood of NSVT compared with those without this finding (28% vs. 4%), and the presence of two-dimensional strain, which is used to identify myocardial fibrosis, in more than three left ventricular segments is an independent predictor of NSVT.121,122
Clinical and Prognostic Significance
The physician who cares for a patient presenting with an episode of NSVT has two tasks. First, he or she needs to establish whether the underlying occult pathology is responsible for the arrhythmia; second, in a case of diagnosed heart disease, the patient should be risk stratified to determine the appropriate management and therapy. The clinical approach to the patient with NSVT should therefore always be considered within the particular clinical context in which the arrhythmia occurs. In several settings, the patient with NSVT represents a clinical challenge with regard to proper management, and several crucial questions remain unanswered.123 The occurrence of an abrupt ventricular arrhythmia is a multi-factorial process involving a continually changing complex substrate of myocardial scarring, ischemia, and adrenergic and genetic factors. We are therefore dealing with a probabilistic event in which each of the currently considered risk factors such as NSVT identifies only a small fraction of the risk process.
The independent prognostic significance of NSVT depends on the underlying condition (Table 43-2). It currently is not known whether NSVT bears a cause-and-effect relationship with sustained ventricular tachyarrhythmias or if it is merely a surrogate marker of left ventricular dysfunction and electric instability. Even when it does hold prognostic significance, NSVT does not necessarily imply the mechanism of death. Certain patient groups have a high mortality rate because of the progression of their disease. Death in these patients may be arrhythmic, but this does not imply that mere prevention of NSVT will unconditionally prolong life significantly. The cardiac mortality rate at 2 years in MADIT was still 11% despite the use of defibrillators.10 Furthermore, reduction of arrhythmic death does not necessarily imply a concomitant reduction in total mortality, and even a nonsignificant increase in mortality has been demonstrated despite the reduction of SCD by using amiodarone in patients with acute MI.124–126
Table 43-2 Clinical Significance of Nonsustained Ventricular Tachycardia
| CLINICAL SETTING | SIGNIFICANCE |
|---|---|
| APPARENTLY NORMAL HEART | |
| Random finding | No adverse prognostic significance in the absence of occult pathology |
| During or after exercise | May predict IHD and increased cardiac mortality |
| Valvular disease, hypertension | Prognostic significance unknown |
| ISCHEMIC HEART DISEASE | |
| Acute MI <13–24 h | No adverse prognostic significance |
| Acute MI >13–24 h | Adverse prognostic significance |
| Chronic IHD with LVEF >40% | Unknown. No adverse prognostic significance(?) |
| Chronic IHD with LVEF <40% | Adverse prognostic significance |
| DCM | Independent prognostic significance not established as opposed to LVEF |
| HCM | Adverse prognostic significance, especially in the young |
| Long QT syndrome, CPVT, repaired congenital abnormalities | Adverse prognostic significance |
| ARVC, Brugada syndrome | Probably adverse prognostic significance |
ARVD, Arrhythmogenic right ventricular cardiomyopathy; CPVT, catecholaminergic polymorphic ventricular tachycardia; DCM, dilated cardiomyopathy; HCM, hypertrophic cardiomyopathy; IHD, ischemic heart disease; LVEF, left ventricular ejection fraction; MI, myocardial infarction; VF, ventricular fibrillation.
Apparently Healthy Individuals
Early reports from longitudinal community-based studies indicated that the presence of complex ventricular ectopy and NSVT increase the risk of heart disease subsequently observed.15 In other studies, NSVT was not found to adversely influence prognosis, with cardiac event rates not exceeding those detected in age-matched populations without the arrhythmia.16,40 Polymorphic NSVT, as opposed to monomorphic NSVT, may indicate an increased risk.127 Thus, recording of spontaneous NSVT in apparently healthy individuals does not imply an adverse prognosis, provided that occult cardiomyopathy and genetic arrhythmia disorders have been excluded. These conditions, however, may remain latent for several years, and although apparently healthy individuals presenting with NSVT can be reassured about their prognosis, long-term follow-up is advisable.
NSVT originating from the RVOT may occasionally cause syncope, although the risk of death is very low. Short cycle length during NSVT and a history of syncope are predictors of the coexistence of VF and polymorphic VT.128 Subjects with RVOT VT might have subtle structural and functional abnormalities of RVOT as detected by CMRI.129 Detection of NSVT in patients with ARVD indicates intermediate risk for future arrhythmic events.130 The diagnosis of RVOT VT needs to be differentiated from the diagnosis of ARVD or cardiomyopathy, which can be accomplished by a series of noninvasive ECG and imaging studies such as Holter monitoring, SAECG, CMRI and, if needed, endomyocardial biopsy.81
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


