Mechanism of Tachycardias
Most cardiac arrhythmias can be described as abnormalities of impulse formation, impulse conduction, or a combination of both. For example, the ventricular premature complex (VPC) which initiates monomorphic ventricular tachycardia in a patient with a prior anterior myocardial infarction represents an abnormality of impulse formation whereas the scar-mediated reentrant ventricular tachycardia is a manifestation of abnormal impulse conduction.
Triggered activity and abnormal automaticity, two common mechanisms of arrhythmia, are categorized as disorders of impulse formation.
Triggered Activity
Triggered activity is the development of firing of a cluster of myocardial cells triggered by a series of preceding impulses. It is generated by a series of afterdepolarizations, which are spawned from a reduced level of membrane potential. These oscillations in membrane potential, if they reach threshold potential, can trigger the development of specific arrhythmias. Afterdepolarizations that develop before the completion of repolarization (during phase 2 or 3 of the action potential) are called early afterdepolarizations (EADs). Afterdepolarizations which occur following repolarization are called delayed afterdepolarizations (DADs) (see Fig. 3-1).
EADs are believed to be responsible for arrhythmias associated with the acquired and congenital long QT syndromes. Slow heart rates and long coupled intervals promote the development of EADs, whereas faster heart rates and shorter coupled intervals suppress EADs. The administration of magnesium may suppress the development of EADs, explaining its effect in the management of polymorphic VT secondary to a prolonged QT interval (torsades de pointes).
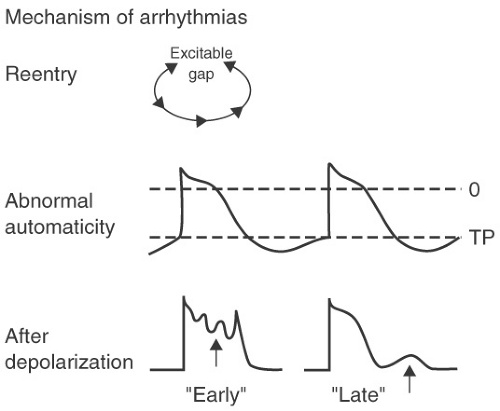 FIGURE 3-1. Different mechanisms of tachycardias. |
DADs are felt to arise from transient inward currents which trigger membrane depolarizations. These transient inward currents occur in response to intracellular calcium overload and subsequent calcium release from the sarcoplasmic reticulum. DADs are due to an inward current produced by the Na/Ca exchanger. DADs have been demonstrated in tissue exposed to digitalis and many of the digoxin-associated arrhythmias are felt to be due to triggered activity. Accelerated idioventricular rhythms following myocardial infarction are also likely due to calcium loading and DADs resulting in triggered activity.
Clinical presentation (see Table 3-1): Clinical clues that an arrhythmia is due to triggered activity include the development of a tachycardia following an increase in sinus rate. The most common example is idiopathic right ventricular outflow tract tachycardia occurring in the setting of exercise or in response to a β-agonist and felt in many instances to be due to DADs.
Response to electrophysiologic study
Overdrive acceleration: This refers to the observation that in rhythms due to triggered activity (due to DADs) when the heart is paced at a rate greater than the tachycardia rate the tachycardia rate increases following cessation of pacing (see Table 3-2).
TABLE 3-1 Mechanism of Common Clinical Arrhythmias
Reentry
Triggered Activity
Automaticity
APD, atrial premature depolarization; DAD, delayed after depolarization; AVNRT, atrioventricular nodal reentrant tachycardia; RVOT, right ventricular outflow tract; VT, ventricular tachycardia; AVRT, atrioventricular reentrant tachycardia; LQT, long QT; EAD, early after depolarization.
Atrial tachycardia (initiates w/APD)
Atrial tachycardia (paroxysmal and associated with block e.g., digoxin toxicity due to DADs)
Atrial tachycardia (warms up, incessant younger patients)
AVNRT
RVOT VT
Reperfusion VT
AVRT
LQT (EADs)
Ischemic VT
Atrial flutter
VT (scar mediated)
Fascicular VT
Idiopathic VT (verapamil sensitive)
TABLE 3-2 Influence of Electrophysiologic Study (EPS) and Drugs on Different Mechanisms of Tachycardia
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


