Chapter 23 Limitations and Uses of the ECG
Important Limitations of the ECG
Like most clinical tests the ECG yields both false-positive and false-negative results, as previously defined. A false-positive result is exemplified by an apparently abnormal ECG in a normal subject. For example, prominent precordial voltage may occur in the absence of left ventricular hypertrophy (LVH) (see Chapter 6). Furthermore, Q waves may occur as a normal variant and therefore do not always indicate heart disease (see Chapters 8 and 9). In other cases, Q waves may be abnormal (e.g., due to hypertrophic cardiomyopathy) but lead to a mistaken diagnosis of myocardial infarction (MI).
False-negative results, on the other hand, occur when the ECG fails to show evidence of some cardiac abnormality. For example, some patients with acute MI may not show diagnostic ST-T changes, and patients with severe coronary artery disease may not show diagnostic ST segment depressions during stress testing (see Chapter 9).
Utility of the ECG in Special Settings
Although the ECG has definite limitations, it often helps in the diagnosis of specific cardiac conditions and sometimes aids in the evaluation and management of general medical problems such as life-threatening electrolyte disorders (Box 23-1). Some particular areas in which the ECG may be helpful are described here:
ST segment elevation in right chest precordial leads (e.g., V4-6R) in a patient with acute inferior infarction indicates associated right ventricular ischemia or infarction (see Chapter 8).
Persistent ST elevations several weeks after an MI should suggest a ventricular aneurysm.
A new S1Q3T3 pattern or right bundle branch block (RBBB) pattern, particularly in association with sinus tachycardia, should suggest the possibility of acute cor pulmonale resulting from, for example, pulmonary embolism (see Chapter 11).
Low QRS voltage in a patient with elevated central venous pressure (distended neck veins) and sinus tachycardia suggests possible pericardial tamponade. Sinus tachycardia with electrical alternans is virtually diagnostic of pericardial effusion with tamponade (see Chapter 11).
LVH is seen in most patients with severe aortic stenosis or severe aortic regurgitation.
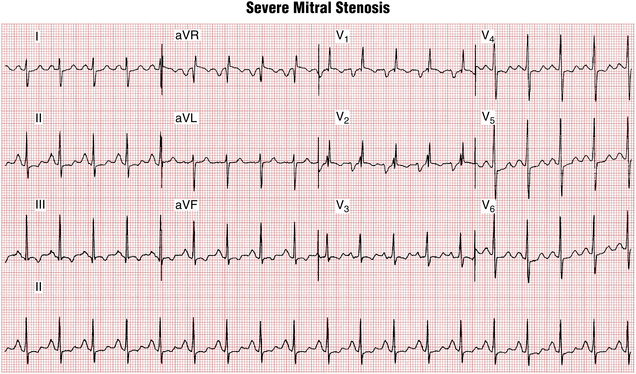
ECG signs of left atrial enlargement (abnormality) with concomitant RVH strongly suggest mitral stenosis (Fig. 23-1).