Fetal Heart Rate Patterns Associated with Fetal Central Nervous System Dysfunction
For some time it has been known that fetal heart rate (FHR) patterns preceding hypoxic fetal death in utero have characteristics that are not usually found in well-oxygenated fetuses or in fetuses with hypoxia that is not severe and/or prolonged (1,2,3,4,5 and 6). Martin et al. (7) have shown that with progressive fetal hypoxemia, late deceleration is first produced by a central nervous system (CNS) reflex that can be inhibited by autonomic blockade. When hypoxia advances to a point where significant fetal acidemia occurs, however, FHR variability disappears and one can no longer inhibit late deceleration with autonomic blockade. We therefore know that severe hypoxemia and acidosis are capable of altering CNS responsiveness and that this is reflected in the FHR pattern. Similarly, it is well established that fetuses with severe nonhypoxic CNS abnormalities may have FHR patterns that differ from those in babies with intact CNSs (8,9,10,11 and 12). Because the ultimate goal is the prevention of fetal CNS damage from intrauterine hypoxia, we must examine what we have learned about FHR patterns associated with CNS dysfunction. Furthermore, recent research shows that maternal infection with chorioamnionitis and funisitis may result in cytokine-mediated CNS dysfunction and damage (see Chapter 3), and it is our recent experience that FHR patterns found in this condition may also reflect CNS dysfunction without preceding FHR patterns known to be associated with fetal hypoxia. FHR monitoring cannot truly determine whether preexisting brain damage was present at the time fetal monitoring was initiated. The patterns described in this chapter, fortunately, are not common and have not been studied in a systematic fashion, and we therefore depend on somewhat anecdotal accounts.
When the modulatory function of the CNS is impaired, a lack of variability is the most common effect seen in the FHR pattern (10). However, other changes are observed when CNS control is impaired (13). Many of these changes are also seen in very premature fetuses in which, presumably, the brain is less well developed. They can also occur when the mother has taken drugs that affect the fetal brain (14,15,16,17,18 and 19). Interestingly, FHR evidence of CNS dysfunction in anencephalic fetuses varies with the level of the defect, from normal to severely abnormal (8,20). It would appear that when a sufficient amount of cerebral cortex and midbrain is present in anencephalic fetuses, FHR variability may be normal and accelerations may be present. However, with no midbrain or cortex present, variability is absent. When the fetus has a complete heart block or when there is a supraventricular fetal tachycardia caused by an ectopic pacemaker not under CNS control, there will also be a complete lack of variability (10).
As more experience is gained with FHR pattern observation in fetuses that subsequently show CNS damage as neonates, it is increasingly clear that the patterns preceding birth are often more characteristic of a lack of CNS control than of ongoing hypoxia. Certainly, these same characteristics are seen in fetuses with CNS dysfunction resulting from acute ongoing hypoxia, and fetuses with chronic oxygen deprivation may also show evidence of CNS dysfunction in the FHR prior to labor. Therefore, while we recognize that preexisting CNS insults or abnormalities may produce changes in the FHR indicating CNS dysfunction, these same changes may accompany FHR patterns indicating ongoing hypoxia (late deceleration or severe variable deceleration); it is not possible to determine the degree of CNS dysfunction that is preexisting and the degree of dysfunction that is due to an ongoing hypoxic process. It should also be pointed out that not all fetuses with CNS abnormalities will have signs of CNS dysfunction on the FHR monitor strip.
The following FHR patterns are evidence of fetal CNS dysfunction:
FLAT FETAL HEART RATE
When CNS dysfunction is present, there may be virtually no fluctuation in the FHR pattern (Figs. 13.1,13.2,13.3,13.4,13.5 and 13.6). This change does not occur in cycles lasting 20 to 40 minutes, as are observed in cases of fetal state change. We are often restricted to external FHR recordings and, as a result, cannot be absolutely sure that short-term variability is absent; however, with the newer autocorrelation method (see Chapter 4), we can get a better idea of short-term variability. Long-term variability (three to five cycles per minute) is reduced or absent, and if present, takes on a very smooth shape (Fig. 13.4).
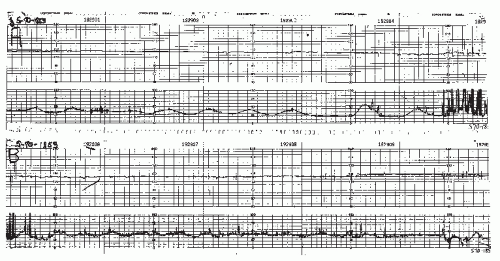 Figure 13.1. A flat fetal heart rate pattern with no periodic changes. It could be due to a preexisting central nervous system (CNS) abnormality, drugs, or, occasionally, a fetus with CNS dysfunction and ongoing hypoxia.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|